Friday Stats and More
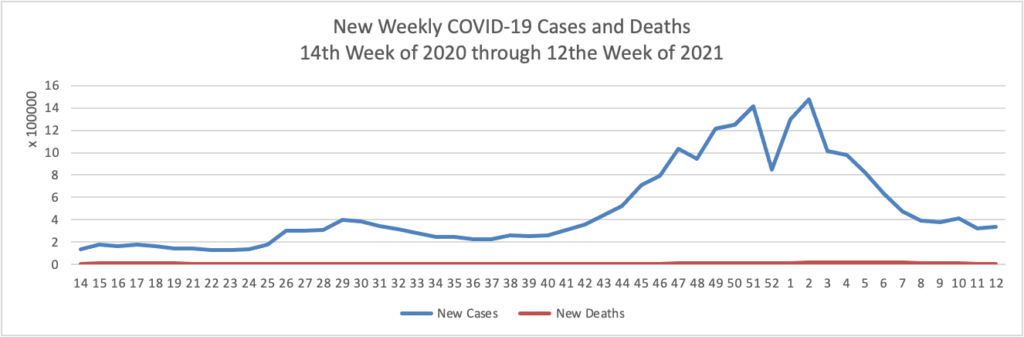
Based on the Centers for Disease Control’s COVID-19 Data Tracker website, here is the FEHBlog’s chart of new weekly COVID-19 cases and deaths over the 14th week of 2020 through 12th week of this year (beginning April 2, 2020, and ending March 24, 2021; using Thursday as the first day of the week in order to facilitate this weekly update):
and here is the CDC’s latest overall weekly hospitalization rate chart for COVID-19:

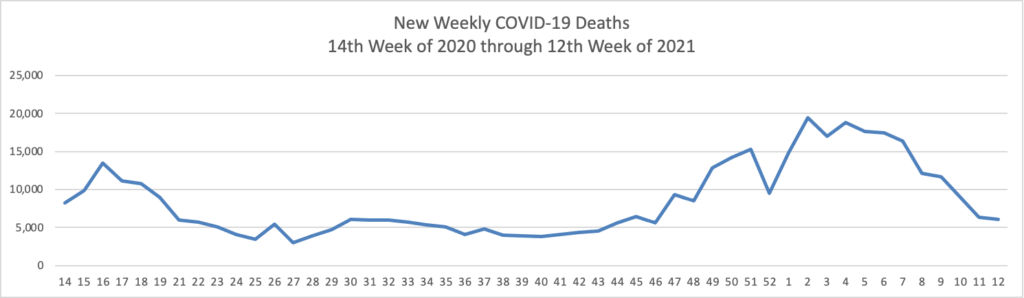
The FEHBlog has noticed that the new cases and deaths chart shows a flat line for new weekly deaths because new cases greatly exceed new deaths. Accordingly here is a chart of new COVID-19 deaths over the period (April 2, 2020, through March 24, 2021):
Finally here is a COVID-19 vaccinations chart for the past three months which also uses Thursday as the first day of the week:
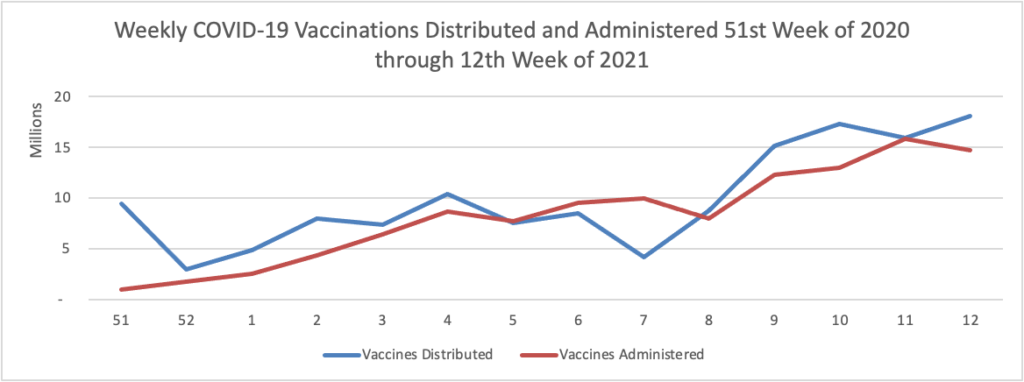
The charts continue to look pretty good. As of today 34.6% of the U.S. population over 18 years old has received at least one dose of the COVID-19 vaccine and 46% of the U.S. population over 65 years old is fully vaccinated.
STAT News reports that
Pfizer and BioNTech said Thursday they are beginning a study aimed at showing their Covid-19 vaccine can be used in children as young as 6 months.
The study follows the launch of a separate and ongoing trial in children ages 12 to 15, which was fully enrolled in January. That study could lead to results by the end of the first half of the year, depending on the data, and then to an emergency use authorization. That will depend on the Food and Drug Administration and the Centers for Disease Control and Prevention. The vaccine already has an EUA for people 16 and older.
“The FDA, if it sees fit to do this, could, grant an EUA and get them into children in that age group by the fall, provided the CDC also agrees and that that should be the vaccine they receive,” said William Gruber, Pfizer’s senior vice president of vaccine clinical research and development.
Moderna began a similar study of their vaccine on children from age 6 months to 12 years old on March 16.
STAT News also offers “A user’s guide: How to talk to those hesitant about the Covid-19 vaccine.” Here’s one good idea:
Have a conversation
Don’t lecture your family and friends, and don’t assume you know what their concerns are. Make sure to listen.
“Try to address their concerns, not what you assume are their concerns,” said Jorge Moreno, an internist and assistant professor at the Yale University School of Medicine. While you may be thinking people are ensnared in the darkest of conspiracy theories, many may have concerns that are much simpler to address. For Moreno, who even had to convince his mother the vaccine was safe, many questions he’s received have centered around side effects, and whether they might make people too sick to work. A Carnegie Mellon University survey released this week showed 70% of vaccine-hesitant people were concerned about side effects.
“Let people know it’s OK to have questions and that having concerns is legitimate,” added Reed Tuckson, the former public health commissioner for Washington, D.C., and a founding member of the Black Coalition Against Covid, which co-developed a campaign called “The Conversation” to provide Black families credible vaccine information. “Letting people have a safe space to have this conversation is essential,” he said. “Wagging your finger against someone is not very useful.”
From the tax front:
- The Internal Revenue Service recently announced that “amounts paid for personal protection equipment, such as masks, hand sanitizer and sanitizing wipes, for the primary purpose of preventing the spread of the Coronavirus Disease 2019 (COVID-19 PPE) are treated as amounts paid for medical care under § 213(d) of the Internal Revenue Code (Code). * * * Group health plans, including health FSAs and HRAs, under the terms of which expenses for COVID-19 PPE may not be reimbursed, may be amended pursuant to this announcement to provide for reimbursements of expenses for COVID-19 PPE incurred for any period beginning on or after January 1, 2020, and such an amendment will not be treated as causing a failure of any reimbursement to be excludable from income under § 105(b) or as causing a § 125 cafeteria plan to fail to meet the requirements of § 125.”
- What’s more, Spotlight on Benefits explains how the IRS has clarified Pandemic-Related Relief for Dependent Care FSAs.
In healthcare business news, Healthcare Dive explains why being a hospital chief financial officer is a particularly tough job during the pandemic. Also Fierce Healthcare discusses a CIGNA telehealth study finding that
while virtual visits for other types of services declined after the initial COVID-19 spike, virtual visits for behavioral health remained in high demand. In April 2020, virtual visits made up about 50% of claims for non-behavioral health services and declined over the course of the year to account for nearly 25% today.
“Virtual behavioral health care is not only a way to access mental health services in the wake of social distancing, but it also allows us the option to pursue treatment in the privacy and comfort of our own homes,” Lustig said.
By contrast, in April, 66% of office visits for behavioral health were conducted virtually, and it’s remained largely flat since.
Behavioral telehealth users also reported higher productivity at work, according to the survey. These patients reported a 45% decrease in sick days, compared to a 28% decrease in miss workdays among patients who did not use telehealth.
That’s good news for the spoke and hub telehealth companies and for health plans and consumers because the spoke and hub telehealth network therapists are in-network.