Friday Stats and More
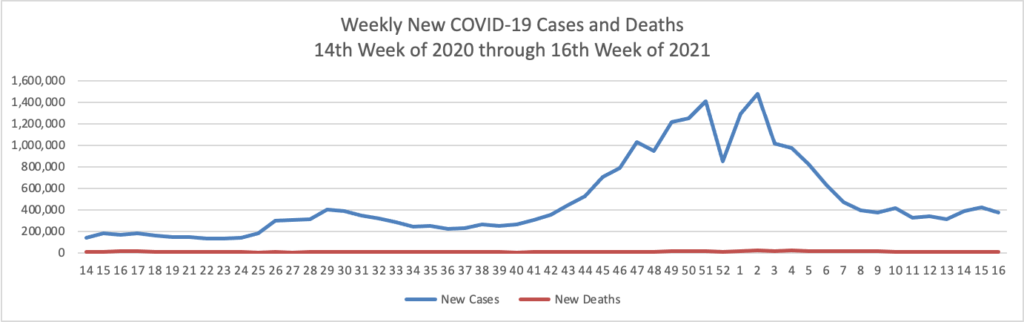
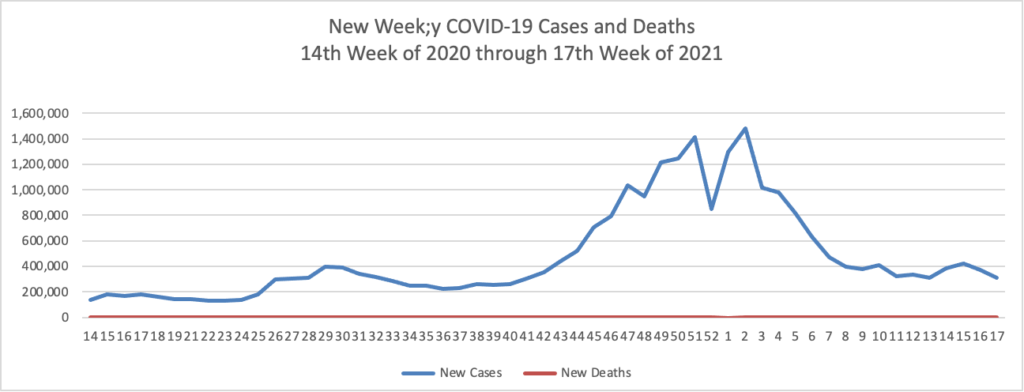
Based on the Centers for Disease Control’s COVID-19 Data Tracker website, here is the FEHBlog’s chart of new weekly COVID-19 cases and deaths over the 14th week of 2020 through 17th week of this year (beginning April 2, 2020, and ending April 28, 2021; using Thursday as the first day of the week in order to facilitate this weekly update):
and here is the CDC’s latest overall weekly hospitalization rate chart for COVID-19:

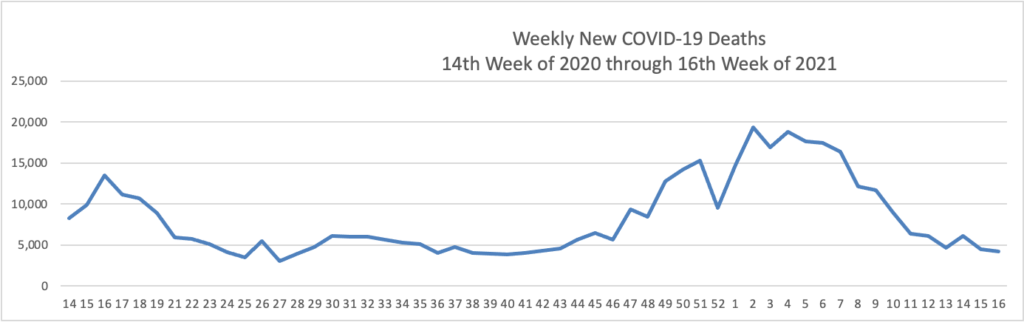
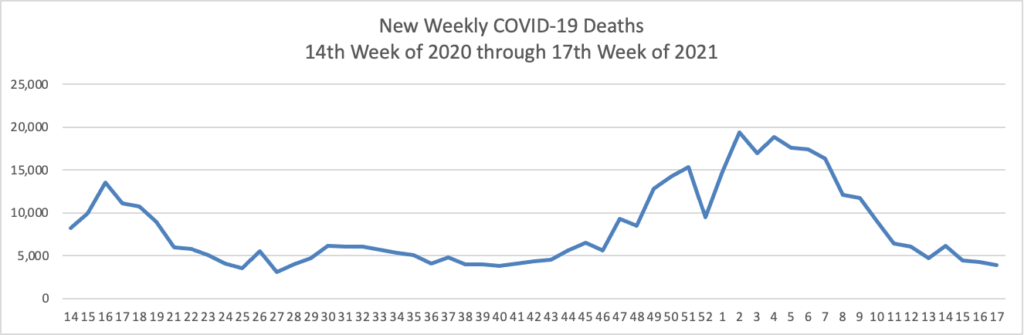
The FEHBlog has noticed that the new cases and deaths chart shows a flat line for new weekly deaths because new cases greatly exceed new deaths. Accordingly here is a chart of new COVID-19 deaths over the period (April 2, 2020, through April 28, 2021):
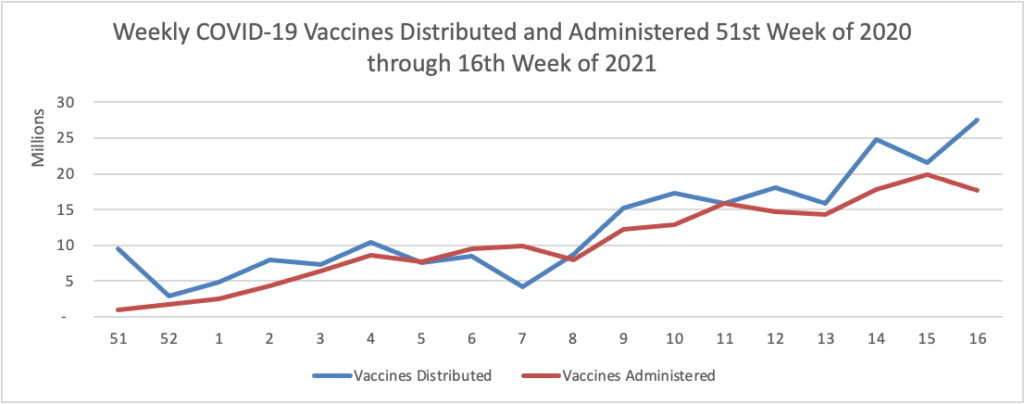
Finally here is a COVID-19 vaccinations chart over the period December 17, 2020, through April 28, 2021 which also uses Thursday as the first day of the week:
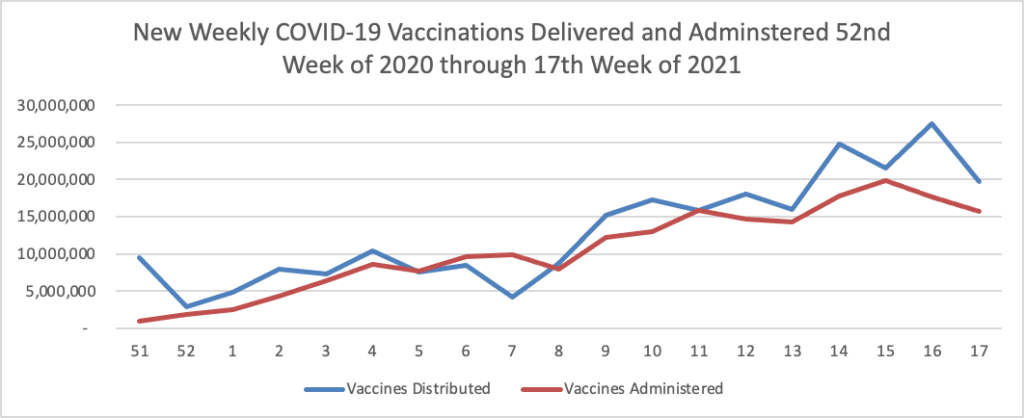
As of yesterday, 39% of the U.S. population over age 18 and 68.8% of those over age 65 have been fully vaccinated. The Centers for Medicare & Medicaid Services Office of Minority Health will host a May 13 webinar on building COVID-19 vaccine confidence. Register for the 12 p.m. ET webinar here. The FEHBlog already has done so.
The American Hospital Association reports that “The Centers for Medicare & Medicaid Services today released a second final notice of benefit and payment parameters to implement standards governing health insurance issuers and marketplaces for 2022 that were not finalized in the Jan. 19 final rule. CMS chose not to finalize the proposed premium adjustment percentage and instead finalized a lower percentage, resulting in lower maximum out-of-pocket costs for consumers ($8,700 for individuals and $17,400 for families) than originally proposed.” These are the 2022 out of pocket maximums on in-network cost sharing that apply to FEHB plans. Here’s a link to the HHS press release which promises even more guidance down the road.
The Centers for Medicare and Medicaid Services announced the winner and runner-up in its healthcare artificial intelligence competition today. “Out of more than 300 initial entries, ClosedLoop.ai was chosen as the grand prize winner and will receive up to $1 million in prize money. Based in Austin, Texas, the company is a leader in developing healthcare data science solutions. Challenge Runner-Up Geisinger, a non-profit healthcare system based in Danville, Pennsylvania [and the carrier of an FEHB plan], will receive up to $230,000 in prize money.” Congratulations.