From the Omicron and siblings front, Fortune Well explores earlier pandemics for similarities to our current one.
As U.S. COVID czar Dr. Anthony Fauci and colleagues pointed out in a 2009 New England Journal of Medicine article, “It is not generally appreciated that descendants of the H1N1 influenza A virus that caused the catastrophic and historic pandemic of 1918–1919 have persisted in humans for more than 90 [now 100] years and have continued to contribute their genes to new viruses, causing new pandemics,” including the 2009 H1N1 “swine flu.”
“We are living in a pandemic era that began around 1918,” they wrote 13 years ago—long before the advent of COVID-19.
“They change and hopefully they adapt and behave,” Brüssow said. “But there are still some escapes, and we might see a return with higher virulence. Vigilance is indicated.”
Pfizer Inc. expects demand for its Covid-19 antiviral drug to increase as governments return to replenish their supplies and seek to thwart surges as the pandemic virus continues to evolve.
The treatment, a pill called Paxlovid, brought in $1.5 billion in sales during Pfizer’s first quarter, while its vaccine totaled $13.2 billion, reflecting the need for tools to combat the virus despite a slowdown in cases and a growing sense of life trying to return to normal.
The company said Tuesday it is on track to deliver between $98 billion and $102 billion in revenue for the year, with $32 billion coming from its Covid-19 vaccine Comirnaty and $22 billion from Paxlovid.
“We remain bullish on Paxlovid” said Chief Financial Officer Frank D’Amelio on a call discussing earnings with analysts. “The rhythm of that product looks very good.”
Biogen is replacing CEO Michel Vounatsos, the company said Tuesday, ending a five-year tenure in which he presided over the disastrous approval and rollout of its Alzheimer’s treatment, Aduhelm.
The company also said it is “substantially eliminating” all spending on Aduhelm just 10 months after securing U.S. approval — a concession from the struggling biotech that the drug had become a financial liability following a Medicare decision to restrict patient access and payment.
From the Affordable Care Act front, Health Affairs Forefront features the third and final part of Katie Keith’s series on the final 2023 notice of benefit and payment parameters. The third part discusses changes to the ACA marketplace’s risk adjustment program.
From the No Surprises Act, the FEHBlog had understood that the NSA regulators planned to release a final rule on the NSA’s arbitration process, replacing the interim final rule, this month. However, a Justice Department filing with the U.S. Court of Appeals for the Fifth Circuit submitted late last week states, “the Departments expect to issue a final rule early this summer that will supersede the portions of the interim final rule that Plaintiffs [in the Texas Medical Association case] challenged.” No wonder then that the final rule has not been presented yet to OMB’s Office of Information and Regulatory Affairs for its required review before publication in the Federal Register.
Agencies’ hiring efforts for the Bipartisan Infrastructure Law (IIJA) are “foot to the pedal,” OPM Director Kiran Ahuja said in an exclusive interview with Federal News Network.
The surge includes filling 3,000 of those new positions over the first six months after President Joe Biden signed the bill into law.
Ahuja has frequently spoken about her goals to attract more early-career workers to federal service. The BIL gives OPM another chance to do just that.
FedSmith identifies four personal budget factors Federal retirees must anticipate. One of those factors is our beloved FEHBP.
The CDC offers ten tips for coping with diabetes distress.
From the No Surprises Act front, the FEHBlog nearly fell off his chair when he noticed this Healthcare Dive article:
The Department of Justice intends to appeal a federal judge’s ruling that sided with providers over a challenge to the surprise billing rule, according to a Friday filing from the DOJ in the Eastern District of Texas.
The Texas Medical Association sued the federal government over its interpretation of the No Surprises Act, arguing the rule leans too heavily on one factor arbiters are supposed to consider when resolving payment disputes between payers and providers.
Federal Judge Jeremy Kernodle’s February ruling said nothing in the bill passed by Congress instructs arbiters to “weigh any one factor … more heavily than the others,” indicating the rule conflicts with the bill.
The Justice Department noticed an appeal to the Fifth Circuit in the referenced Friday, April 22, filing with the District Court. That notice effectuates the appeal. The FEHBlog will keep an eye on the dockets to learn whether the Justice Department will seek a stay of the February ruling while the case is on appeal.
From the Omicron and siblings front —
Bloomberg’s Prognosis reviews progress being made in the development of Covid vaccines administered nasally. Nasal vaccines have a better shot at preventing COVID than injected vaccines.
The American Hospital Association reports “The Food and Drug Administration today expanded its approval for remdesivir (Veklury) to include pediatric patients under age 12 who test positive for SARS-CoV-2 and are hospitalized or at high risk of progressing to severe COVID-19. The patient must be at least 28 days old and weigh at least 3 kilograms (about 7 pounds). FDA said the approval is supported by a clinical study of 53 pediatric patients as well as trials in adults, given the similar course of disease in adult and pediatric patients.”
Medical Dialogues informs us the World Health Organization has recommended Pfizer’s Paxlovid Covid pill over remdesvir, Merck’s pill and monoclonal antibodies for patients with milder forms of Covid and nevertheless at high risk of hospitalization from the disease, e.g. the elderly, the immunocompromised, and the unvaccinated.
WebMD News tells us “COVID-19 was the third-leading cause of death in the United States in 2021 for the second straight year, with only heart disease and cancer causing more deaths, the CDC said Friday. * * * The overall number of COVID deaths in 2021 increased around 20% over 2020, when around 384,000 people died from the virus, the CDC said. COVID deaths in 2021 peaked for the weeks ending Jan. 16 and Sept. 11, following holiday periods.”
The WebMD article offers other interesting public health nuggets. For example,
About 693,000 people died of heart disease in 2021, with 605,000 dying of cancer and 415,000 of COVID, the CDC said, citing provisional data that might be updated later.
Unintentional injuries were the fourth-leading cause of death, increasing to 219,000 in 2021 from 201,000 in 2020. Influenza and pneumonia dropped out of the top 10 leading causes of death and suicide moved into 10th place.
Overall, about 3,458,697 deaths were reported in the U.S. last year. The age-adjusted death rate was 841.6 deaths per 100,000 people, an increase of .7% from 2020. The 2021 death rate was the highest since 2003, the CDC said.
From the healthcare business front, Fierce Healthcare reports
Change Healthcare has found a buyer for its payment integrity arm, ClaimsXten, though the sale is contingent on the closure of its merger with UnitedHealth Group.
According to a filing submitted Monday to the Securities and Exchange Commission, ClaimsXten will be sold off to an affiliate of TPG Capital for a base purchase price equal to $2.2 billion in cash. UnitedHealth is listed as the seller.
From the reports department —
The National Bureau of Economic Research offers a working paper titled “Pharmacy Benefit Managers and Vertical Relationships in Drug Supply: State of Current Research.”
Per HR Morning, “Employer support [of their workforces] is happening in the areas of increased prioritizing employee assistance programs (EAPs), expanded wellness benefits and greater attention to work/life balance. That’s according to Ragan’s 2022 Communications Benchmark Report that surveyed close to 1,000 communicators across industries on opportunities and changes.”
Per Health Payer Intelligence, Humana has produced an issue brief that provides “an overview of the policymaking landscape surrounding social determinants of health data collection.”
The Centers for Disease Control and Prevention on Wednesday asked the Justice Department to appeal a federal judge’s ruling overturning the federal mask mandate for airlines and other forms of public transportation, setting up a legal battle that could permanently impact the CDC’s ability to weigh in on public health issues.
The judge’s ruling was the latest in a series of court decisions that have left the Biden administration with dwindling legal options for mandates to combat Covid-19. And it came amid a shift away from mask mandates in the U.S., even in Democratic-controlled states along the East and West coasts. An appeal gives the Biden administration the opportunity to persuade a higher court to wipe the Florida ruling off the books, which could prove useful to the White House if it chooses to pursue a mask mandate in the future.
A new U.S. government center [residing within the CDC] aims to become the National Weather Service for infectious diseases — an early warning system to help guide the response to COVID-19 and future pandemics.
The new Center for Forecasting and Outbreak Analytics launched Tuesday. Its leaders say predicting the course of the COVID-19 pandemic in the U.S. has been hampered by data-collection problems.
In contrast, the United Kingdom uses regular population sampling with swab tests and blood draws to get a clearer picture of who’s been infected, said Marc Lipsitch, the new center’s science director. He said similar sampling should be considered in the U.S.
And the Centers for Disease Control and Prevention needs to have better access to data from state governments and hospitals, said Caitlin Rivers, the center’s associate director.
From the Omicron front, STAT News discusses six Covid mysteries that scientists are beginning to unravel.
Hospitalization rates for unvaccinated children ages 5 to 11 were twice as high as among those who were vaccinated during the record COVID-19 surge caused by the Omicron variant, according to a U.S. study released on Tuesday.
For every 100,000 unvaccinated children in the age group, 19.1 per were hospitalized with COVID-19 between mid-December and late February, compared with 9.2 per 100,000 vaccinated kids, the U.S. Centers for Disease Control and Prevention reported.
From the Social Determinants of Health front,
The Center for Medicare Services “outlined an action plan that demonstrates the Biden-Harris Administration’s ongoing efforts to provide high-quality, affordable health care for all people, regardless of their background, and to drive health equity across the Department of Health and Human Services (HHS).”
“The goals of CMS’ action plan include:
Promoting culturally and linguistically appropriate services in organizations;
Enrolling more people in Medicare, Medicaid, the Children’s Health Insurance Program and Health Insurance Marketplace; and
Incorporating screening for and promoting broader access to health-related social needs.”
The CDC’s Division of Diabetes Translation called attention to its new website on improving health equity
From the No Surprises Act front, the American Medical Association offers an article on how doctors can use the NSA to resolve billing disputes. It’s always helpful to take a peek at the other sides’s strategies.
Beginning in August, Kaiser Permanente commercial HMO and exclusive provider organization (EPO) members who need urgent care when they are traveling outside of areas served by Kaiser Permanente will have access to Cigna’s national PPO network of more than one million physicians and other providers. This will significantly expand Kaiser Permanente’s ability to provide more affordable and convenient access to valuable, high-quality health care and services for current and future members.
This is a smart move by KP to reduce its exposure to NSA emergency department billing disputes.
In the area of specialty pharmacy services, the agreement seeks to deliver overall value and savings to Kaiser Permanente and its commercial plan members. Accredo, Evernorth’s specialty pharmacy, will become Kaiser Permanente’s preferred external pharmacy for limited distribution drugs, and Evernorth’s CuraScript SD will be a preferred distributor for purchasing certain other specialty products.
The broad agreement between Evernorth and Kaiser Permanente is effective immediately.
Anthem’s first-quarter profits reached $1.8 billion thanks to strong enrollment in its Medicaid and Medicare Advantage plans.
Anthem, which operates an array of government and commercial health insurance including Blue Cross and Blue Shield plans in 14 states, Wednesday reported first-quarter profits rose 8.4% to $1.8 billion, or $7.39 per share, compared to $1.67 billion, or $6.71 per share, in the year-ago quarter. Revenue rose nearly 17.6% to $38 billion compared to $32,4 billion a year ago.
Anthem’s membership grew by 3.3 million, or 7.5%, to 46.8 million as of March 31, 2022, compared to a year ago.
According to the report, only 4.6% of hospitals were sold over the period. Small hospitals with 26-64 beds were more likely to be acquired than larger hospitals, and hospitals with the greatest negative margins were over twice as likely as those with the highest positive margins to be acquired (8.6% versus 3.0%). Only one critical access hospital was acquired during the study period, and urban hospitals were more likely to be acquired than rural hospitals (5.6% versus 3.3%). Long-term care hospitals were the most likely to be acquired, while psychiatric and “other” hospitals were the least likely.
The agency plans to update the data on a quarterly basis.
When comparing the use of telehealth among different pediatric subspecialties, a JAMA Network Open study found that pediatric telehealth use was inconsistent across subspecialties, with genetics and behavioral health subspecialists using the care modality the most.
The study included 549,306 patients, representing a total of 1.8 million visits from eight pediatric medical groups from the Children’s Specialty Care Coalition (CSCC). There were 11 different subspecialties, including cardiology, orthopedics, urology, nephrology, dermatology, genetics, behavioral health, pulmonology, endocrinology, gastroenterology, and neurology. The study period began Jan. 1, 2019, and ended Dec. 31, 2021.
Scientists around the world are discovering and tracking newer forms of the Omicron coronavirus variant, showing how even when a strain becomes globally dominant, it continues to evolve and can splinter into different lineages.
Case in point: Updated data released Tuesday showed that a burgeoning form of Omicron, called BA.2.12.1 — itself a sublineage of the BA.2 branch of Omicron — now accounts for nearly one in five infections in the United States. It’s eating into the prevalence of the ancestral BA.2, highlighting the emergent virus’s transmission advantage over its parent. BA.2 now accounts for about 74% of cases, while the remaining 6% or so are from the BA.1 branch of Omicron, the first form of the variant that took over globally and whose prevalence has been falling as BA.2 became dominant.
The menagerie can be dizzying to track, especially because all these cases technically fall under the Omicron umbrella. But even as scientists closely monitor the divergence of Omicron, early signs suggest the different lineages don’t substantially differ in terms of how virulent they are or in their ability to evade the protection generated by immunizations. While some of the newer forms of the virus might be better spreaders than others, their emergence doesn’t necessarily result in huge increases in cases.
David Leonhardt adds in his New York Times morning column today
In several places where the number of cases has risen in recent weeks, hospitalizations have stayed flat. (In past Covid waves, by contrast, hospitalizations began rising about a week after cases did.) * * *
Even if hospitalizations do rise in coming weeks, a declining share of coronavirus cases that result in serious illness would be very good news, Dr. Craig Spencer, director of global health in emergency medicine at Columbia University, has pointed out.
I haven’t seen a Covid patient in the E.R. in weeks and go to work now expecting not to,” Spencer told me, “despite a swirl of Covid in the community.”
Among other things, a decoupling of cases and severe illness would mean that hospitals were less likely to become overwhelmed during future Covid surges. When hospitals avoid getting swamped, they can provide care to every patient who needs it — which becomes another factor that reduces bad health outcomes.
For these reasons, Mr. Leonhardt plans to shift his focus from new cases to new hospitalizations.
Because mRNA-based vaccines are a relatively new class of vaccines, they do not include the traditional adjuvants. The current mRNA vaccines used in the U.S. rely on small balls of fat called lipid nanoparticles to deliver the mRNA. These lipid molecules can act as adjuvants, but how precisely these molecules affect the long-term immune response remains to be seen. And whether the current COVID-19 vaccines’ failure to trigger strong long-lived antibody response is related to the adjuvants in the existing formulations remains to be explored.
While the current vaccines are highly effective in preventing severe disease, the next phase of vaccine development will need to focus on how to trigger a long-lived antibody response that would last for at least a year, making it likely that COVID-19 vaccines will become an annual shot.
New data from Moderna offer hope that booster shots against Covid-19 could become at least somewhat more effective than they already are. But the data also point to how difficult it could be to determine exactly which Covid shots to give as annual boosters.
At a hearing of a Food and Drug Administration advisory panel earlier this month, experts fretted about exactly how governments should make decisions about the composition of annual boosters. And they were adamant that governments, not pharmaceutical companies, should be deciding the strain composition of the shots, as the World Health Organization does for influenza shots. But these data are a reminder that those decisions can be tough. What would experts do when faced with booster shots with several different compositions? Will adding new strains work similarly for different types of vaccines? There are a huge number of open questions.
There’s also the biggest problem with annual flu shots: People don’t get them. Even with the current Covid boosters, this has been true. Data presented to the FDA panel said that 217 million Americans are vaccinated about Covid. But only 90 million people have received a booster dose. How many will turn out for a new booster next year?
Look at this comparison of winter 2019-2020 flu vs. 2020-2021 Covid
2019 – 2020 Winter CDC Fluview
3/28/20
2020-2021 Winter COVID-19
10/1/2020 to 3/21/2021
Flu Deaths
24,000
COVID-19 Deaths
332,636
Flu Cases
39,000,000
COVID-19 cases
22,399,598
Deaths over total cases
0.06%
1.49%
https://www.cdc.gov/flu/weekly/index.htm
Who would look back on pre-Covid flu as the good old days? But comparatively, it is. We see millions more flu cases, but hundreds of thousands fewer flu deaths.
Kaiser Health News discusses the need for better ventilation in office buildings which could help tamp down Covid and flu cases. “The science is airtight,” said Joseph Allen, director of the Healthy Buildings program at Harvard University’s T.H. Chan School of Public Health. “The evidence is overwhelming.”
From the No Surprises Act front, Healthcare Dive reports
The online portal for resolving payment disputes between payers and providers for certain out-of-network charges is now open, the CMS said Monday. The portal initiates what’s known as the federal independent dispute resolution process, a key part of the No Surprises Act that outlaws balance bills in most cases. As a last resort, it allows payers and providers to resolve payment disputes using an arbitration style similar to the model adopted by Major League Baseball in salary negotiations.
From the transparency in coverage rule front, the Labor Department issued ACA FAQ 53 today. FAQ 53 provides guidance to health plans, including FEHB plans, on how to post three machine-readable pricing files on their website. The Labor Department will begin to enforce this requirement on July 1, 2022.
Commercial health plans pay higher prices than public payers for hospital care, which accounts for more than 5 percent of US gross domestic product. Crafting effective policy responses requires monitoring trends and identifying sources of variation. Relying on data from the Healthcare Provider Cost Reporting Information System, we describe how commercial hospital payment rates changed relative to Medicare rates during 2012–19 and how trends differed by hospital referral region (HRR). We found that average commercial-to-Medicare price ratios were relatively stable, but trends varied substantially across HRRs. Among HRRs with high price ratios in 2012, ratios increased by 38 percentage points in regions in the top quartile of growth and decreased by 38 percentage points in regions in the bottom quartile. Our findings suggest that restraining the growth rate of HRR commercial hospital price ratios to the national average during our sample period would have reduced aggregate spending by $39 billion in 2019.
Seniors save nearly $2,000 on average a year in total healthcare spending in Medicare Advantage (MA) compared to fee-for-service Medicare, a new study finds.
The study, published Tuesday, by the advocacy group Better Medicare Alliance finds that seniors spent $1,965 less including premiums and out-of-pocket costs on MA when compared to fee-for-service.
“We see particularly strong results for historically disadvantaged populations, including Black and Hispanic beneficiaries and those who are low-income,” said Allison Rizer, principal at the consulting firm ATI Advisory, which performed the study that examined 2019 Medicare Current Beneficiary Survey data.
From the healthcare business front, Fierce Healthcare tells us
UnitedHealth Group executives said Thursday that its Optum Health subsidiary, which is one of the country’s largest physician groups, is building out value-based care partnerships at a faster rate than was expected.
In its earnings report, the healthcare giant said it initially projected that 500,000 new patients would be treated in value-based arrangements. It’s upping that projection to 600,000. Wyatt Decker, M.D., CEO of Optum Health, said on the company’s earnings call that reflects Optum’s efforts to invest in technology, analytics and building networks are paying off.
“What you’re really seeing is a result of almost 10 years of building a flywheel that now has significant momentum,” Decker said. “All of that continues to yield benefits and, frankly, growth.”
The severity of multiple sclerosis (MS) was linked with geographic latitude, an observational study showed.
Among 46,000 MS patients living in temperate zones, more severe disease was seen in those who lived above 40° latitude, reported Tomas Kalincik, MD, PhD, of the University of Melbourne, Australia, and co-authors.
The association was driven mainly, but not exclusively, by ultraviolet B (UVB) radiation exposure contributing to both MS susceptibility and severity, the researchers wrote in Neurology.
AHRQ discusses a study on “Geographic Variation in Inpatient Stays for Five Leading Substance Use Disorders, 2016-2018.” There are interesting State variations.
From the Omnicron and siblings front, the Wall Street Journal reports encouraging news.
The Omicron BA.2 variant has dominated new infections in the U.S. for weeks without setting off a major surge so far, raising hopes among some public-health experts that the nation might dodge a more significant hit.
BA.2 is in particular affecting the Northeast, where virus concentrations in wastewater are rising alongside reported infections in such places as New York, Washington, D.C., and Philadelphia. Concern about BA.2 prompted Philadelphia to restore an indoor-mask requirement and U.S. authorities to extend mask mandates for airplanes and other forms of transportation.
Still, BA.2 hasn’t yet caused the rise in hospitalizations some doctors said they would have anticipated. Disease experts say some combination of immunity from Covid-19 vaccinations and a severe wintertime surge, aided by springtime weather drawing people outdoors, might be keeping the virus at bay.
A booster dose of the Pfizer-BioNTech COVID-19 vaccine was safe and produced an immune response in kids ages 5 to 11, including against the Omicron variant, the companies said on Thursday.
These data came from two sources: the phase II/III clinical trial on 140 children ages 5 to 11 who received a booster dose at least 6 months after their two-dose primary series, and a subgroup of 30 kids in whom response against Omicron was studied specifically. In this subgroup analysis, there was a 36-fold increase in neutralizing antibody titers compared with levels seen after the two-dose primary series, the companies reported.
The companies plan to submit a request to the FDA for an emergency use authorization (EUA) for a third dose for this age group “in the coming days.” The agency previously authorized a two-dose primary series of the 10 μg formula for this age group in October 2021.
Health IT Analytics tells us, “When comparing groups that experienced the worst effects of COVID-19, a study published in Public Health Nursing found that the pandemic had a significant impact on those who exhibit high social vulnerability, leading them to have the highest mortality levels.” This finding illustrates the importance of resolving health disparities.
More than 90 federal agencies released their first-ever equity action plans on Thursday, laying out more than 300 strategies to better help underserved communities. This follows an executive order President Biden issued on day one of his administration, which directed agencies to conduct equity assessments of their top three to five high-impact services for Americans to determine where there were systematic barriers. These findings helped agencies develop their plans.
“Taken together these 300 actions demonstrate what it means to take a whole-of-government approach to advancing equity,” said a senior administration official on a background briefing call. “For the first time Americans will see a full picture of what it looks like for the entire federal government to advance equity at once.”
In a significant development from the No Surprises Act front, the Affordable Care Act regulators issued helpful Federal Independent Dispute Resolution (IDR) Process Guidance for Disputing Parties and Certified IDR Entities. The new guidance no longer treats the Qualifying Payment Amount as a rebuttable presumption. This action strongly suggests that the QPA’s rebuttable presumption status will be removed from the “final, final” version of the IDR rule. That regulation is due out next month. However, the rule does not yet appear on the OMB Office of Information and Regulatory Affairs’ list of rules currently being subjected to their oversight.
In other regulatory news, the International Foundation of Employee Benefits Plans alerts us,
The Department of Justice (DOJ) released guidance including frequently asked questions (FAQs) on how the Americans with Disabilities Act (ADA) protects individuals from discrimination when they are being treated for and recovering from opioid use disorder (OUD).
A group of 30 bipartisan lawmakers sent letters to 7 naloxone manufacturers, calling on them to apply for over-the-counter status for their opioid overdose antidotes and open up supplies further as the opioid crisis continues in the US with record levels of overdoses and deaths.
Citing a Massachusetts study that found substantially increased access to naloxone reduced opioid overdose mortality rates by 46%, the senators and representatives called on Pfizer, Teva Pharmaceuticals, Adamis Pharmaceuticals, Akorn, Amphastar Pharmaceuticals, Emergent BioSolutions, and Hikma Pharmaceuticals to “submit applications to make naloxone available over the counter without delay.”
Currently, there are three FDA-approved forms of naloxone — injectable, auto-injector and nasal spray — and all three currently require a prescription, but in most states and the District of Columbia pharmacists are allowed to dispense naloxone under a standing order, meaning they don’t actually need individual prescriptions. Some states also have given pharmacists direct authority to prescribe and sell naloxone to consumers.
Good idea. The HHS Secretary Xavier Becerra extended the opioid epidemic public health emergency for another 90 days earlier this month.
From the healthcare business front, Healthcare Dive reports on UnitedHealth Group’s 1st Quarter 2022 financial results.
UnitedHealth is bullish on completing its controversial acquisition of data analytics firm Change Healthcare, despite legal action from the Department of Justice to block the deal.
UnitedHealth’s extended agreement with Change “reflects our firm belief in the potential benefits of this combination to improve healthcare and in our ability to successfully overcome the challenge to this merger,” Chief Operating Officer Dirk McMahon told investors on a Thursday morning call regarding first-quarter financial results.
The Minnetonka, Minnesota-based healthcare behemoth beat Wall Street expectations for earnings and revenue in the quarter, with a topline of $80.1 billion, up 14% year over year due to double-digit growth at health services arm Optum and payer business UnitedHealthcare. Net earnings were $5.1 billion, up 3% year over year. UnitedHealth raised its full-year guidance following the results.
The Omicron surge didn’t lead to an explosion of medical claims at UnitedHealth Group, which contributed to higher-than-expect profits. UnitedHealth ended the first three months of the year with more than $5 billion of profit on $80.1 billion of revenue. The company’s medical loss ratio, which shows the percentage of insurance premiums that were spent on medical claims, was 82% — higher than 80.9% in the first quarter of 2021, but less than what Wall Street expected.
From the miscellany department
The ICD 10 Monitor discusses “two extremely encouraging studies in terms of the content coverage and feasibility of replacing ICD-10-CM with ICD-11.”
BioPharma Dive reports “AbbVie and Genmab said treatment with their dual-acting antibody epcoritamab led to responses in nearly two-thirds of patients with lymphoma, announcing on Wednesday that their clinical trialsurpassed its benchmark for success. The partners will now take the data to the Food and Drug Administration and other regulators to determine whether it’s good enough to formally submit for approval.”
Health Data Management offers useful insights into the ongoing TEFCA launch.
From the Capitol Hill front, today, the Senate took the following action
PN1166: Krista Anne Boyd, of Florida, to be Inspector General, Office of Personnel Management– Considered by Senate.– Confirmed by the Senate by Voice Vote.
And just like that, OPM has a Senate-confirmed Inspector General for the first time in over six years. The FEHBlog wishes Inspector General Boyd good luck.
The President issued a statement on World Health Day, which was celebrated today.
From the Omicron and siblings front —
The Centers for Medicare Services released an updated Toolkit on Covid Vaccines for health insurers and Medicare Advantage plans.
A federal appeals court has reinstated President Biden’s COVID-19 vaccine mandate for the federal workforce, overturning a lower court’s nationwide pause that had been in effect since January.
The plaintiffs who brought their suit over Biden’s executive order did not have standing in the federal circuit, a panel of the U.S Court of Appeals for the Fifth Circuit said in a 2-1 opinion Thursday evening, and instead must pursue their appeals through the Merit Systems Protection Board or Office of Special Counsel as laid out in the Civil Service Reform Act. The court vacated the injunction and instructed the district court in Texas that issued it to dismiss the case upon remand.
Medicare on Thursday finalized its plan to restrict coverage for the controversial, pricey Alzheimer’s drug Aduhelm to patients participating in clinical trials.
The decision marks the end of an intense pressure campaign from drugmakers and some patient groups who wanted Medicare to reverse its initial proposal and pay for the drug for more patients. As clinical trials are usually run out of major medical centers, the decision will likely mean some interested patients won’t be able to access the drug. However, Medicare isn’t explicitly requiring that patients be treated at hospital-based clinics like the initial proposal.
The decision has implications beyond Aduhelm’s manufacturer, Biogen, as well. The coverage decision is not specific to Aduhelm, and applies to all drugs in the class, including a forthcoming treatment that Eli Lilly has begun to submit for FDA approval.
But in a major change from the initial proposal, Medicare officials created a sort of shortcut path for drugs that, unlike Aduhelm, demonstrate a clinical benefit for patients before they are approved. Medicare will cover those medicines for a broader group of patients.
They would still need to collect some data, but the possible design of the studies is much more flexible — a significant win for Lilly.
Here is a link to the CMS fact sheet on this decision.
U.S. News adds “Medicare said Thursday it’s considering a cut in enrollee premiums after officials stuck with an earlier decision to sharply limit coverage for a pricey new Alzheimer’s drug projected to drive up program costs.” Given Medicare’s shaky financial condition, one would expect the government to build up reserves with the additional cash and then adjust the premium for the following Medicare year, taking all considerations into account.
From the No Surprises Act front, AHIP released a new resource reflecting on the first 100 days of the NSA.
From the healthcare business front, Fierce Healthcare informs us
[Blue Cross of California and Walgreen] are launching new Health Corners in 12 Walgreens stores in the San Francisco Bay area and Los Angeles County.
At the Health Corner locations, Blue Shield members and customers will be able to connect with health advisers who can offer simple in-store care as well as assistance with preventive screenings, chronic care management and medications. The health advisers have clinical backgrounds, such as pharmacists or nurse practitioners.
The partnership seemed a natural fit, D.D. Johnice, vice president of the Health Transformation Lab at Blue Shield of California, said in an interview. * * * Some 80% of people in California live within five miles of a Walgreens store, she said, so the Health Corners could be a valuable tool for reaching people who live in healthcare deserts, or more specifically, Blue Shield network deserts.”
Michael F. Neidorff, who as chief executive officer of Centene Corp. transformed a tiny medical insurance firm serving three counties in 1996 into a nationwide giant in government-backed health coverage, died Thursday after what his family described as a long illness. He was 79.
Mr. Neidorff recently took medical leave and had signaled last year a plan to retire in 2022 from the CEO job he held for more than 25 years. Centene announced in March the appointment of Sarah London, who had been vice chairman, to succeed him as CEO.
St. Louis-based Centene is the biggest company in managed Medicaid, contracting with states to provide coverage to people enrolled in the program for lower-income Americans.
Centene offers FEHB HMO coverage through its Health Net subsidiary. RIP.
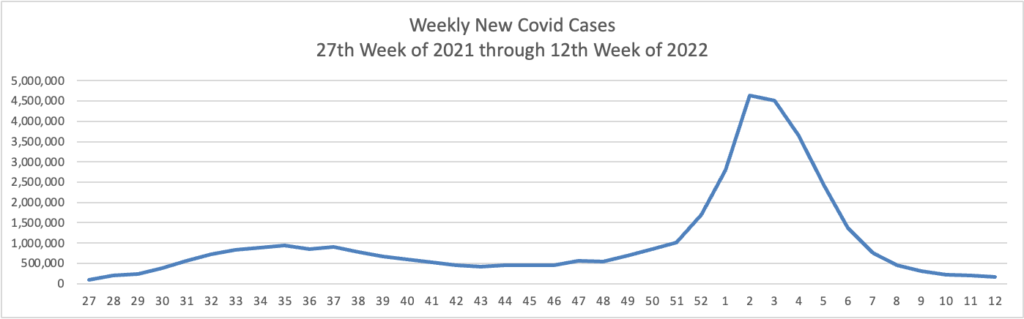
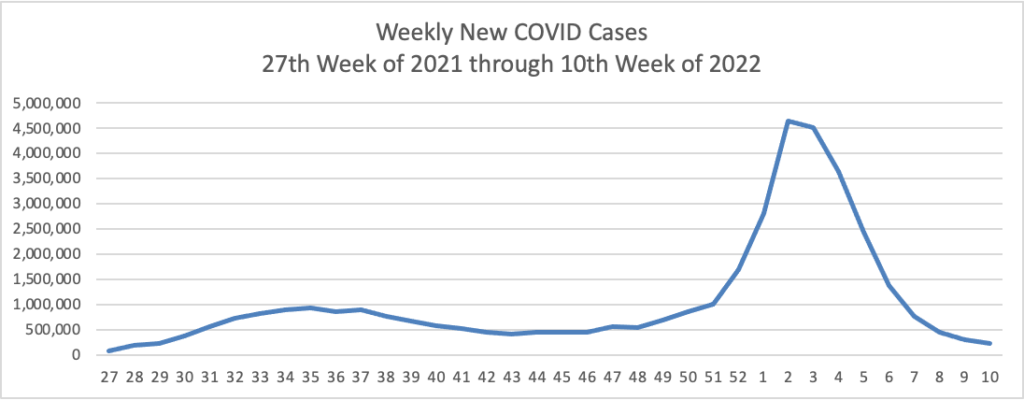
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s weekly chart of new Covid cases from the 27th week of 2021 through the 12th week of 2022:
In the current CDC Covid Data Weekly Tracker, the CDC explains
In February, CDC’s COVID Data Tracker released a Wastewater Surveillance tab, which tracks changes and detections of SARS-CoV-2 viral RNA levels at more than 600 testing sites across the country. Because many people with COVID-19 shed the virus in their feces, wastewater testing can help us monitor COVID-19 in communities. Virus levels in wastewater usually increase four to six days before clinical cases increase, so surveillance results can help communities act quickly to prevent the spread of COVID-19.
Currently, virus levels in wastewater are relatively low across the country. More than half of all sites reporting wastewater data are experiencing a decrease in SARS-CoV-2 levels, but some have reported a modest uptick. These upticks may reflect minor increases from very low levels to levels that are still low. It’s important to note that even a small increase when levels are very low can appear like a dramatic increase in the percent change. However, there is a possibility that some communities might start to see an increase in COVID-19 cases. This could happen for a variety of reasons, like waning immunity, new circulating strains, and eased prevention strategies.
Right now, it’s too early to know if we’ll see a corresponding increase in reported cases across the country. Wastewater data are meant to be used with other COVID-19 surveillance data. CDC encourages local public health officials to watch for sustained increasing levels of the virus in wastewater, and to use wastewater surveillance data with other kinds of data to inform their decisions. CDC continues to encourage people to use COVID-19 Community Levels to find out what actions they should take to protect themselves and others. The whole community can be safe only when we all take steps to protect each other.
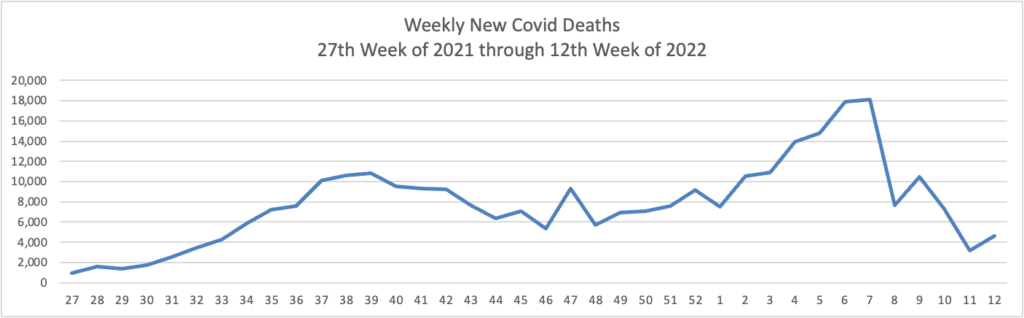
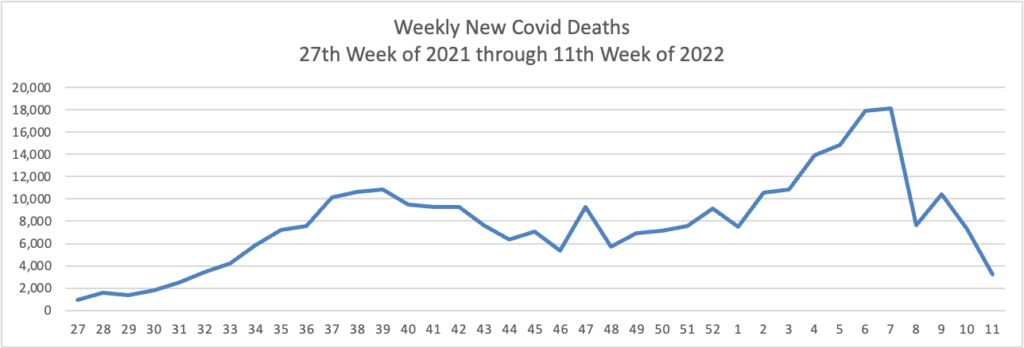
Using the same approach, here is the FEHBlog’s latest weekly chart of Covid deaths:
[T]he 2022 trend data from the CDC indicates pneumonia may soon overtake COVID-19 as the leading cause of respiratory death in the U.S.
Historically, the CDC reported the number of visits to emergency departments with pneumonia as the primary diagnosis averaged about 1.5 million, which led to 47,000 deaths annually.
The good news is pneumonia is a vaccine-preventable disease.
Unfortunately, the percentage of adults who had ever received a pneumococcal vaccination was 25.5% in 2020.
Increasing the pneumococcal vaccination rate is a worthy goal for health plans and primary care providers.
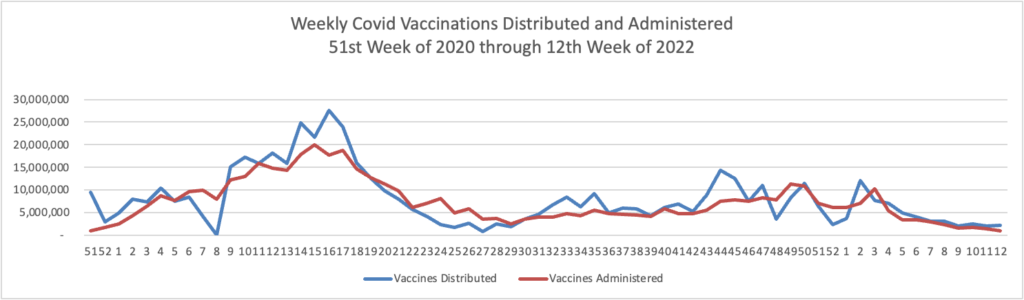
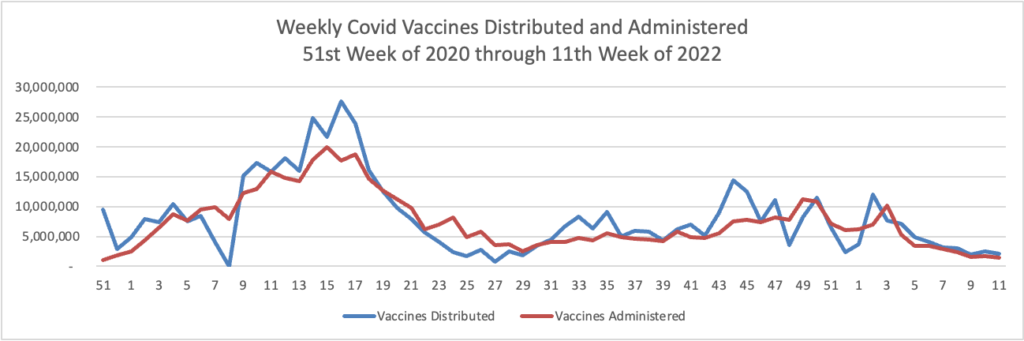
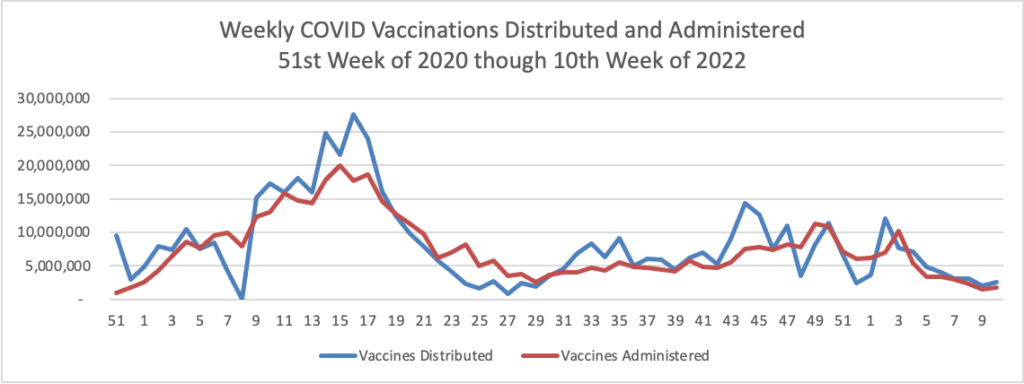
Here’s is the FEHBlog’s weekly chart of Covid vaccinations distributed and administered in the Covid vaccination era:
While recent vaccinations numbers are nothing to crow about, over 75% of Americans age 18 and older are fully vaccinated. Nearly half of the same population and over two-thirds of Americans age 65 and older have received a booster.
The Biden administration could authorize a second Covid-19 booster shot for older Americans within weeks, amid rising concern over a potential resurgence of cases, four people with knowledge of the matter told POLITICO.
The move under consideration by senior health officials would recommend the additional vaccine dose for adults 65 and older, in an effort to better protect high-risk people and stave off a wave of hospitalizations should infections climb rapidly as a result of the spread of the Omicron subvariant, BA.2. Currently, second boosters are only recommended for those with compromised immune systems.
From the No Surprises Act front, last Monday, Federal District Judge Richard Leon heard oral argument on dispositive cross-motions submitted by medical associations and the federal government regulators concerning the status of the qualifying payment amount in the baseball arbitration process. The FEHBlog has heard from a couple of sources who attended the hearing that Judge Leon indicated that he does not plan to put deciding the case on his front burner because the federal regulators advised him about their intent to issue the final, final rule on the Independent Dispute Review process in May 2022. The case is pending in the U.S. District Court for the District of Columbia.
From the telehealth front, mHealth Intelligence informs us
More than two-thirds of telehealth providers said they use audio-only modalities to offer telehealth services, according to a recent survey conducted by the American Medical Association.
The survey polled 2,232 physicians between Nov. 1 and Dec. 31, 2021.
The popularity of telehealth among physicians is apparent, with 85 percent saying they still use it. But 52 percent agreed that their telehealth usage has decreased since they first started offering the services. The top reason for the decrease was that they moved to a hybrid model of care with both in-person and virtual care services.
The company confirmed the deal in a statement to the outlet. The acquisition has not been announced publicly as of yet.
“Optum and Refresh Mental Health are excited to expand effective behavioral care to patients through a more coordinated health system,” the company said in a statement to Axios. * * *
Refresh was founded in 2017 and provides outpatient mental and behavioral health services. It runs 300 locations across 37 states that offer a variety of services including psychiatry and substance abuse treatment.
Bicycle Health, a virtual provider for opioid use disorder, is partnering with five additional payers, it said in an announcement provided exclusively to Fierce Healthcare.
The partnerships are with Molina Healthcare and McLaren Health Plans in Michigan, UHC Community Plan in Arizona, Health First Colorado (the state’s Medicaid program) and Blue Cross Blue Shield Texas. In total, these payer partnerships have the potential to reach more than 8 million patients, the company said. Coverage will include medication management, behavioral health (individual or group psychotherapy, medical care), support groups and care coordination.
“From high costs to significant time commitments, many traditional OUD recovery programs just aren’t realistic options for the vast majority of patient experiences,” Bicycle Health CEO and founder Ankit Gupta said in a statement. “We are committed to making science-based, holistic OUD treatment accessible to all who need it—and these partnerships are an exciting step towards that goal.”
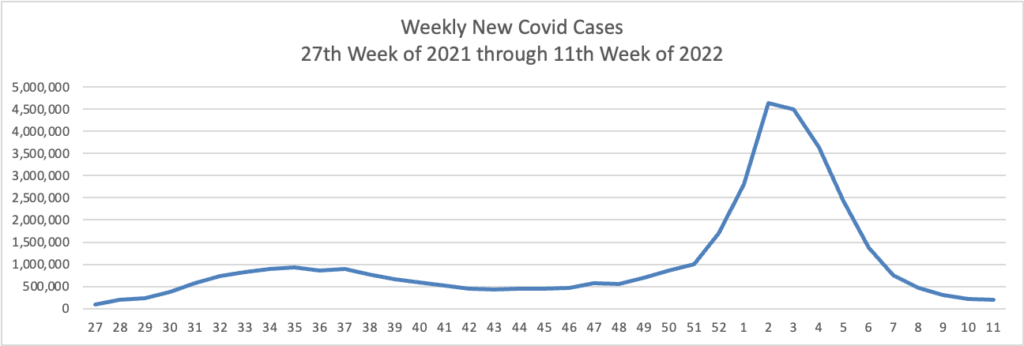
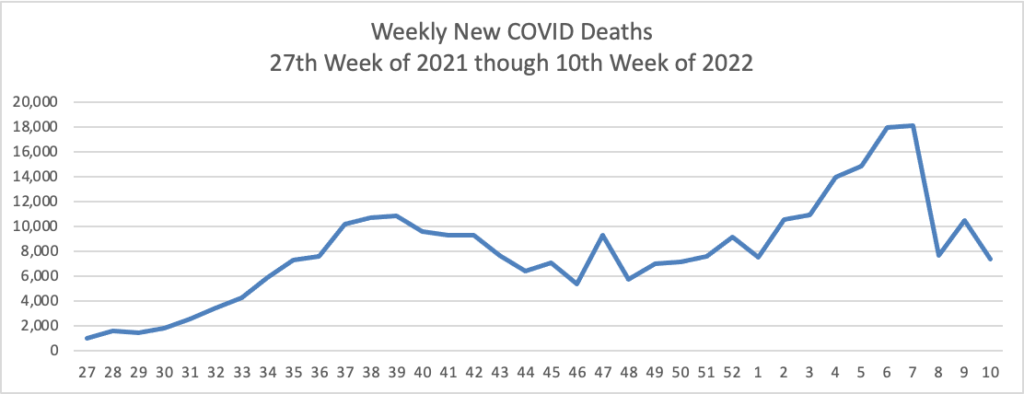
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s latest weekly charts of new Covid cases and deaths (a lagging indicator):
The CDC observes in its weekly review of its Covid statistics
COVID-19 cases, hospitalizations, and deaths all continue to decrease in the United States. According to CDC’s COVID Data Tracker, as of March 16, 2022, 76.7% of the total U.S. population has received at least one dose of a COVID-19 vaccine, and 65.3% has completed their primary series. However, only about half of the booster-eligible population has received a booster dose and is considered up to date on their COVID-19 vaccines.
Two new studies show the effectiveness of COVID-19 vaccines and boosters across periods of three variants of concern (Alpha, Delta, and Omicron). CDC released a study today showing that, among adults hospitalized with COVID-19 during the Delta and Omicron waves, those who received two or three doses of the Pfizer-BioNTech or Moderna vaccine had 90–95% less risk of dying or needing a ventilator compared with adults who were not vaccinated. Protection was highest in adults who received a third COVID-19 vaccine dose. A study published in the British Medical Journalexternal icon found that vaccines gave a high level of protection against hospitalization for all variants, but not as much for Omicron among adults who received only a primary series. However, boosters increased protection against Omicron. The study also showed that hospital patients who were vaccinated had much lower disease severity than patients who were not vaccinated.
These studies emphasize the importance of staying up to date with vaccinations—they are our best protection against severe COVID-19 illness. Vaccination is also the safest way to reduce the chance that new variants will emerge. Find a vaccine provider and get your booster dose as soon as you can.
In that regard, here is the FEHBlog weekly chart of Covid vaccinations distributed and administered from the beginning of the vaccination era in late 2020:
Here’s a link to the Food and Drug Administration’s March 18 round of its Covid related activities.
While the bulk of Covid care spending goes to hospitals, Becker’s Hospital Review reports that a “sizable minority” have a significant amount out-of-pocket spending for this care, according to a study published in the American Journal of Managed Care March 16.”
It’s worth adding that the Wall Street Journal reports that
The biggest credit-reporting firms will strip tens of billions of dollars in medical debt from consumers’ credit reports, erasing a black mark that makes it harder for millions of Americans to borrow.
Equifax Inc., ExperianPLC and TransUnion are making broad changes to how they report medical debt beginning this summer. The changes, which have been in the works for several months, will remove nearly 70% of medical debt in collections accounts from credit reports.
Beginning in July, the companies will remove medical debt that was paid after it was sent to collections. These debts can stick around on a consumer’s credit report for up to seven years, even if they are paid off. New unpaid medical debts won’t get added to credit reports for a full year after being sent to collections.
The firms are also planning to remove unpaid medical debts of less than $500 in the first half of next year. That threshold could rise, according to people familiar with the matter.
From the compliance front —
The Internal Revenue Services issued a notice on how to calculate the No Surprises Act’s Qualified Payment Amount when the health plan does not have enough data to calculate a January 2019 median.
The Department of Labor is offering a webinar on March 30 at 11 am that “will help employers, service providers, and benefit professionals understand how the provisions of [the federal mental health partity act] apply to employer-sponsored group health plans and provide information on how to avoid common problems. The webinar runs about 45 minutes to an hour and is limited to 200 participants.
From this week’s healthcare conferences front
Fierce Healthcare discusses the electronic medical records interoperability theme of the HIMSS conference.
Fierce Healthcare also offers a wrap report on “the most interesting innovations at SXSW 2022: From holograms to the future of psychedelics.”
From the telehealth front
Becker’s Payer Issues reports that most consumer driven plans have taken advantage of the IRS offered flexibility to cover telehealth before the “high” annnual deductible.
Forbes informs us “Telehealth Accounts For One In Three Mental Health Visits Two Years Into Pandemic.” Whoopee.
From the good works department, the American Medical Association tells us about a North Carolina physician who is talking the diabetes problem.
Dr. [Brian] Klausner is the medical director of WakeMed’s Community Population Health program in Raleigh. He also is a physician champion for DiabetesFreeNC. That is the statewide initiative where AMA partnered with the North Carolina Medical Society and others to support collaborative efforts to end type 2 diabetes in the Tar Heel State.
Rather than think of the pandemic as having “derailed” diabetes prevention or other population health efforts, Dr. Klausner said that “COVID-19 expedited new perspective in how we can do a better job addressing historic roadblocks to community health initiatives, including those related to diabetes and prevention.”
From the FEHB front, the Office of Personnel Management released the 2023 call letter for benefit and rate proposals and the related technical guidance letter.
OPM is to be congratulated for releasing the two letters simultaneously. Historically, OPM has released the call letter weeks or months before the technical guidance letter. As a result, carriers cannot start preparing their benefit and rate proposals, due May 31, until they receive both letters.
From the Omicron (and sibling) front, the American Medical Association informs us
The New York Times (3/15, Mandavilli) reports about “17 million Americans received the Johnson & Johnson Covid vaccine, only to be told later that it was the least protective of the options available in the United States.” However, “new data suggest that the vaccine is now preventing infections, hospitalizations and deaths at least as well as the Pfizer-BioNTech and Moderna vaccines.” The reasons are unclear, “and not all experts are convinced that the vaccine has vindicated itself.” Still, “the accumulating data nonetheless offer considerable reassurance to recipients of the vaccine and, if confirmed, have broad implications for its deployment in parts of the world.”
From the mental health care front, the American Hospital Association tells us
The Substance Abuse and Mental Health Services Administration yesterday released a toolkit to help health care providers and others prepare for the July 16 launch of 988, the new phone number for anyone experiencing suicidal thoughts or a mental health or substance use crisis to speak, text or chat with a trained crisis counselor. Authorized by the National Suicide Hotline Designation Act of 2020, the three-digit number will operate through the National Suicide Prevention Lifeline’s network of over 200 crisis centers.
“In the longer term, our vision is to build a robust crisis care response system across the country that links callers to community-based providers who can deliver a full range of crisis care services, if needed (like mobile crisis teams or stabilization centers),” SAMHSA notes.
To access the toolkit and other suicide prevention resources, visit SAMHSA’s new 988 website.
From the U.S. healthcare front, Healthcare Dive reports
The long-term shift from hospital-based care toward more treatment delivered in the home and ambulatory centers picked up pace during the COVID-19 pandemic and is expected to continue to gain momentum, pressuring revenue growth and margins in the hospital sector, according to new research from Moody’s Investors Service.
Reimbursement changes, risk-sharing, investment in outpatient services including ambulatory surgery centers, advances in drugs and medical devices and greater use of at-home acute care services are among the forces driving the movement away from more expensive hospital inpatient care.
Medicare telehealth visits increased 63-fold during 2020, Moody’s said, citing HHS data. Although hospitals are reporting that telehealth use is receding as more patients return to in-person physician visits, it will likely remain above pre-COVID levels, the ratings agency said.
Kaiser Health News looks at the No Surprises Act from the patient’s perspective. It’s an important article because health plans should help their members keep the new law’s billing protections in perspective.
From the provider of the future front, mHealth Intelligence reports
Though a majority (63 percent) of clinicians worldwide expect most of their consultations to be remote within the next decade, 51 percent believe that telehealth will negatively impact their ability to demonstrate empathy with their patients, a new report revealed.
Developed by Elsevier Health and Ipsos, the Clinician of the Future report includes a quantitative survey, qualitative interviews, and roundtable discussions with nearly 3,000 practicing physicians and nurses worldwide. Of the total number of respondents, 434 were from the US. * * *
Empathy from physicians is becoming increasingly important for patients. A vast majority of clinicians (82 percent) surveyed said that soft skills like listening and displaying empathy have become more critical in the last decade. In the US, 76 percent of clinicians agreed with this statement.
Though the importance of soft skills has grown, the report notes that technical skills will be key in the future.
From the HIMSS Conference in Orlando, Florida, Healthcare Dive holds an interview concerning the FEHBlog leading interoperability innovation of 2022, TEFCA:
Healthcare Dive caught up with Mariann Yeager to talk TEFCA at the HIMSS annual healthcare conference in Orlando on Monday. Yeager is CEO of the Sequoia Project, a nonprofit that was selected in 2019 to serve as the recognized coordinating entity (RCE) charged with developing, updating and maintaining the common agreement and overseeing QHINs.
Yeager shared more details on the timeline of TEFCA implementation, why organizations should join the voluntary framework and how the Sequoia Project and the Office of the National Coordinator for Health IT are at the beginning of a long process of monitoring and modernizing a living document that, given uptake, could shape the future of health data exchange for decades into the future.
“We’re really proud of the work that we’ve done,” Yeager said.
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s updated weekly chart of new Covid cases:
Not quite as low as we were in early July but very much moving in the right direction. So is the FEHBlog’s updated weekly chart of new Covid deaths, which is considered a lagging indicator.
The epidemiologists have a keen eye out for new worrisome variants. For example, for other troubling variants, Becker’s Hospital News tells us about a relatively new combination of Delta and Omicron known as Deltacron.
The recombinant variant appears unlikely to spread as easily as delta or omicron, William Lee, PhD, vice president of science at Helix, told USA Today. “We have not seen any change in the epidemiology with this recombinant,” WHO COVID-19 technical lead Maria Van Kerkhove, PhD, said of deltacron during a March 9 media briefing. “We haven’t seen any change in severity. But there are many studies that are underway.”
Here’s the FEHBlog’s weekly chart of Covid vaccinations distributed and administered from the start of the Covid vaccination era in late 2020 until the week ended this past Wednesday.
It is noteworthy that this week, the percentage of Americans aged 18 and older who are fully vaccinated (two doses of mRNA vaccine) cracked 75%. The same cadre is closing in on being 50% boostered. The most at risk, over age 65 cadre is 89% fully vaccinated and 66.7% boostered.
In a study of 1,364 children aged 5-15, two doses of the Pfizer COVID-19 vaccine reduced the risk of omicron infection by 31% in those under 12 and 59% in older children, the Centers for Disease Control and Prevention reported today. CDC said the study reinforces the importance of vaccination to keep children and teens protected from severe disease, noting that another recent study found the vaccine 92%-94% effective against COVID-19 hospitalization in adolescents during the delta surge and 74% effective against hospitalization in younger children during omicron.
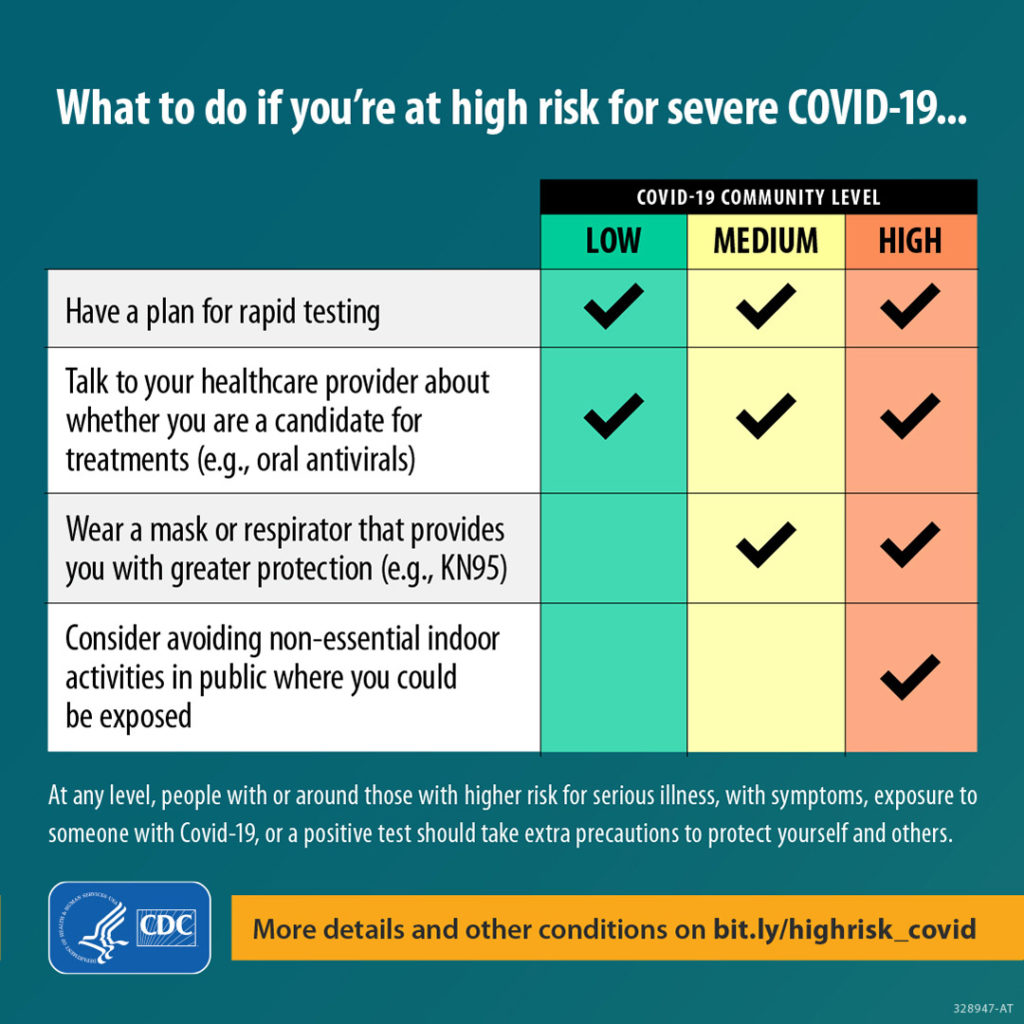
Here’s a link to the CDC’s weekly review of its Covid statistics. This week’s issue focuses on protecting folks at high risk for Covid, such as the immunocompromised.
Who is most likely to become very sick or die from COVID-19? Your chances increase with age and underlying medical conditions like cancer, diabetes, heart conditions, dementia, and obesity, particularly if you’re not up to date on vaccinations. People with weakened immune systems,* some disabilities, some mental health conditions, and some chronic diseases are also at higher risk. A lot of people might not know they’re at risk for severe illness—review the list to find out if you could be.
Here’s a link to the CDC’s weekly Fluview report, which states that flu activity is increasing in “most of the country.” In this regard, the American Medical Association inform us
Healio (3/10, Downey, Gallagher) reports “interim estimates published Thursday in” the CDC’s Morbidity and Mortality Weekly Report “indicate that this season’s influenza vaccine has not been effective.” Based on the data “from more than 3,600 children and adults,” researchers “estimated that the vaccine has been 16% effective against mild or moderate influenza caused by the predominant circulating virus, influenza A(H3N2), with a 95% confidence interval…that suggests vaccination ‘did not significantly reduce the risk of outpatient medically attended illness’ caused by H3N2.”
From Capitol Hill and closing the loop on Thursday’s post, the Senate did pass the fiscal year 2022 omnibus appropriations act Thursday night. Roll Call reports
On a 68-31 vote, the Senate passed the 2,700-page, $1.5 trillion omnibus containing all 12 fiscal 2022 spending bills, $13.6 billion in supplemental appropriations to address the crisis in Ukraine and a lengthy list of unrelated measures fortunate enough to ride on the must-pass vehicle.
From the No Surprises Act front, the FEHBlog had been concerned that the federal regulators were giving up on using the Qualified Payment Amount as a rebuttable presumption in NSA arbitrations which would help tremendously to control out of network benefit and plan legal costs. The FEHBlog therefore was encouraged to find that the federal government has filed a brief with the federal district court for the District of Columbia defending that position in a case raising the same issue. An oral argument on this issue will be heard by District Judge Richard Leon on March 21, 2022, at 3 pm. The FEHBlog will keep an eye on this and the other federal cases raising this issue.
From the electronic health record front, MedCity News interviews the CEO of Epic Systems at the Vive conference. The interview covers interoperability, artificial intelligence and other timely topics.
From the opioid epidemic front, STAT News reports
It was in the mid-2010s, the researchers heard, when “tranq dope” — opioids that contained the veterinary tranquilizer xylazine — took off in Philadelphia. But now, in some places across the U.S., it was appearing in 1 in 5 overdose deaths. A recent study also found the powerful synthetic opioid fentanyl in nearly every xylazine-involved death as well, indicating it wasn’t just the tranquilizer causing these overdoses. Experts are still trying to understand the risks of xylazine, but they’re worried because the drug is not an opioid but acts as a sedative, which can increase the risk of a fatal overdose. It might also make it harder to reverse those overdoses with naloxone, which is designed to work on opioids. STAT’s Andrew Joseph has more on how adulterated — and in turn, increasingly dangerous — the U.S. drug supply has become.
Rur roh.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.