Congressional leaders are set to return to the Capitol on Monday under pressure to negotiate a spending bill that would fund the federal government’s operations beyond Friday.
Negotiators have days to reach a deal on a full-year spending bill or pass a short-term measure delaying the deadline to avoid a partial government shutdown. To reach a longer-term deal, they will have to break the partisan deadlock between Republicans and Democrats, who are split over $26 billion in nondefense spending in talks to craft an omnibus bill. * * *
Senate lawmakers are expected this week to pass a defense policy bill that authorizes U.S. military leaders to purchase new weapons and increase pay for troops, and lifts a requirement for members of the military to get vaccinated against Covid-19.
Tomorrow is the last day of the Federal Employee Benefits Open Season. According to OPM, the official end is 11:59 pm “in the location of your electronic enrollment system”
The FEHBlog noticed on Linked In that OPM Director Kiran Ahuja spoke last week at the Milken Institute’s Future of Health Summit.
Director Ahuja spoke about eradicating stigmas surrounding mental health treatment and creating a welcoming work environment for all.
As the largest employer in the nation, the Federal government must continue to invest in policies, tools, and resources that gives every employee the high quality and accessible mental health supports they need
Hey OPM, why don’t you post the Director’s remarks on opm.gov?
From the infectious disease front, the Secretary of the Treasury has written a letter to the state governors on resources available to combat the tripledemic. The FEHBlog has read articles recommending that we must return to masking and social distancing. The FEHBlog, who is a lawyer, not a health professional, thinks that if we accept this mistaken guidance, we will be tied to masking and social distancing in the winter forever. N.B. This is not a criticism of people who choose to mask social distance. The FEHBlog’s point is that the tripledemic was unavoidable.
From the No Surprises Act (NSA) front, the FEHBlog checked out the docket sheet for the second Texas Medical Association versus the federal NSA regulators challenging the revised final rule implementing the NSA’s independent dispute resolution process without giving the revised rule a chance.
The case is at the cross-summary judgment stage. A summary judgment motion asks the Court to decide the case without a trial because the issues presented are entirely legal.
The federal government filed its motion in early November. The FEHBlog knew the AHIP and employee benefit associations subsequently had filed friends of the court/amici briefs supporting the NSA regulators. The FEHBlog was delighted to read that a group of patient/consumer organizations, including “ALS Association, CancerCare, Epilepsy Foundation, Families USA Action, Hemophilia Federation of America, Leukemia & Lymphoma Society, National Multiple Sclerosis Society, United States Public Interest Research Group, Inc., and Cancer Support Community” also filed an amicus brief supporting the NSA regulators. That is an uplifting amici lineup.
From the U.S. healthcare business front, the Wall Street Journal reports
Amgen Inc. is in advanced talks to buy drug company Horizon Therapeutics PLC. according to people familiar with the matter, in a takeover likely to be valued at well over $20 billion and mark the largest healthcare merger of the year.
The U.S. biotechnology company was the last of three suitors standing in an auction for Horizon, the people said, after French drugmaker Sanofi SA said Sunday it was out of the running.
A deal could be finalized by Monday assuming the talks with Amgen don’t fall apart, the people said.
Horizon develops medicines to treat rare autoimmune and severe inflammatory diseases that are currently sold mostly in the U.S. Its biggest drug, Tepezza, is used to treat thyroid eye disease, an affliction characterized by progressive inflammation and damage to tissues around the eyes.
The company is Nasdaq-listed, but based in Ireland and has operations in Dublin, Deerfield, Ill., and a new facility in Rockville, Md.
From the Federal Employees Benefit Open Season front, Tammy Flanagan, writing in Govexec, explains the relationship between FEHB and Medicare coverage for the benefit of annuitants over age 65.
From the OPM front, Govexec and Federal News Network discuss an OPM management report released yesterday that includes more details on OPM’s 2022 Federal Employee Viewpoint Survey.
From Capitol Hill, Medpage Today informs us that “Telehealth, Mental Health Likely Topics for the New Congress in 2023, Experts Say.” In this regard, today the bipartisan leadership of the Senate Finance Committee “released a [fifth and final mental health parity] discussion draft including policies aimed at improving mental health parity in Medicare and Medicaid and helping to put access to mental health and substance use disorder (SUD) services on par with physical health care. Mental health parity includes a set of laws aimed at ensuring mental and physical health care are covered equally by health insurance. * * * The full text of the discussion draft is available here. A summary of all provisions released by the committee as a part of the bipartisan mental health effort, including mental health parity, is available here.”
COVID-19 hospitalizations have ticked up nationwide in recent weeks amid concerns of a potential winter surge, according to data tracked by The New York Times.
As of Nov. 29, the nation’s daily hospitalization average was 31,125, up 12 percent over the last 14 days. This figure is still down significantly from the more than 800,000 daily hospitalizations recorded during the peak of last winter’s omicron surge.
People with acute respiratory illness during the pandemic suffered similar levels of poor well-being in the months afterward whether they tested positive for SARS-CoV-2 or not, a registry study showed.
In a cohort of people who all had initial symptoms suggestive of COVID-19, those who had moderate to severe scores at 3 months on the pain, mood, and other quality-of-life measures on the Patient-Reported Outcomes Measurement Information System (PROMIS) scale were actually less likely to have tested positive for the coronavirus as to have had other causes of illness (39.6% vs 53.5%, P<0.001).
From the public health front —
MedPage Today explains how patients can try to distinguish among different respiratory illnesses, including RSV and the flu because at home testing is unavailable.
The Biden administration looks to end its public health emergency declaration for mpox — the virus formerly known as monkeypox until recently — a sign that officials believe they’ve brought the unprecedented outbreak under control, POLITICO’s Adam Cancryn reports.
Health officials are likely to issue a 60-day notice later this week for winding down the declaration, two people with knowledge of the matter told POLITICO, putting it on track to expire by Jan. 31. The decision isn’t yet final and could still change, the people cautioned. * * *
Some administration officials see the potential unwinding of the mpox emergency declaration as a test run for eventually ending the yearslong Covid emergency — a more complex challenge — that Biden aides expect to happen at some point next year.
From the Affordable Care Act and No Surprises Act front
The American Hospital Association (“AHA”) informs us
The Centers for Medicare & Medicaid Services seeks public input on topics related to essential health benefits — items and services that all non-grandfathered health plans in the individual and small group markets must cover under the Affordable Care Act. The agency is requesting feedback on how essential health benefits may need to be updated to reflect changes in medical evidence and scientific advancement, address gaps in coverage and health equity, or remove barriers to accessing services. In particular, CMS seeks feedback on essential health benefits related to maternal health, behavioral health and prescription drug coverage. The agency will publish the request for information in the Dec. 2 Federal Register, with comments accepted for 60 days.
and
AHA today urged the Centers for Medicare & Medicaid Services not to establish a national directory of health care providers and services (NDH) at this time.
“The AHA shares CMS’ goals to improve patient access to provider information and to facilitate health information exchange and data reporting,” the association wrote. “We appreciate the commitment CMS has invested in striving to meet these objectives. However, we are concerned that adding one more provider directory requirement will not support patients in accessing the information they need about their care providers. In fact, adding an additional data source without sufficiently addressing how or why it differs from the myriad provider directories already in existence could further complicate patients’ ability to access accurate information. Meanwhile, such a requirement would add considerable, duplicative burden on providers. Additionally, we have significant reservations about the current state of readiness of the essential technology needed for a centralized data hub such as the NDH.”
Mercer Consulting offers insights on the prescription drug and healthcare spending reports that health plans must submit to the federal government by December 27. Jingle bells.
Healthcare Dive reports that the Texas Medical Association has filed another lawsuit challenging different aspect of the independent dispute resolution rule. Haven’t the TMA lawyers heard about the opportunity available under the Federal Rules of Civil Procedure to amend their existing complaint?
The Food and Drug Administration approved the first therapy using bacteria from stool samples to treat a bowel disorder on Wednesday, paving the way for several similar treatments in development.
The drug, called Rebyota, is given as a one-dose treatment for Clostridium difficile infections, commonly known as C. diff., in which the toxin-producing bacteria disrupts the normal balance in a person’s digestive system. Rebyota is designed to restore balance by introducing good bacteria taken from donor stool samples.
“We are delighted that FDA has approved the first fecal microbiome restoration therapy for recurrent C. diff. This is an enormous step forward for the nearly 200,000 people who battle rCDI each year,” said Christian John Lillis, the executive director of the C. diff advocacy organization the Peggy Lillis Foundation.
Amgen released detailed data on Thursday suggesting an early-stage drug can induce significant weight loss in patients with obesity, with less frequent dosing than current treatments but a safety profile that remains unclear.
The results for the molecule, codenamed AMG133, throw Amgen in a long-gestating race with other major drugmakers that burst into the popular press this year.
Eli Lilly and the diabetes giant Novo Nordisk both market drugs that were recentlyshown to lower body weight by around 15% to 20% after a little over a year. (Lilly’s is currently approved only for diabetes, but it plans to submit for obesity next year.) The injectables have been highly sought after by both obesity specialist physicians, who have long searched in vain for something safe and effective to offer their patients, and celebrities hoping to look svelte in their next appearance.
From the miscellany department —
Beckers Hospital Review interviews a Kaiser Permanente expert about their successful use of remotely monitoring patients with diabetes and high blood pressure. The monitors deliver their results to Kaiser Permanente’s electronic health records for 40,000 members. Kudos.
Beckers also lets us know about large hospital systems that are having a profitable 2022.
Elon Musk’s brain-machine interface company Neuralink aims to put its first implant in a human subject in the next six months, he said during an event Wednesday.
Musk said the company has been “working hard to be ready for our first human,” and has submitted most of the required paperwork to the Food and Drug Administration to launch a study in humans. The company — which is designing a device to translate the brain’s signals into actions — also announced it will first focus specifically on two applications: restoring human vision, and helping people who can’t move their muscles to control devices like smartphones or even return the ability to move to people with severed spinal cords, Musk said.
Though it’s starting with certain parts of the brain, Musk said Neuralink’s long-term goal is to create a system that can translate impulses from the entire brain into actions.
Other issues emphasized by Democrats, including passing a ban on the sale of assault-style weapons, are a long-shot given their narrow majority in the Senate. Most legislation requires 60 votes to advance in the Senate. In addition, lawmakers are discussing raising the federal debt ceiling, which limits how much the government can borrow.
Congress faces a Dec. 16 deadline to pass legislation that would continue funding the federal government; failure to do so could result in a partial shutdown. Lawmakers must decide whether to approve a short-term bill or reach a deal on more-detailed legislation that would fund the government for the full fiscal year.
The Senate also will be considering the National Defense Authorization Act, which typically includes government procurement law changes.
Tomorrow, the Federal Employee Benefits Open Season will reach its clubhouse turn with two weeks left to go. Although not a part of the Open Season, Federal News Network reports an important development concerning the Federal Employees Long Term Care Insurance Program (FLTCIP.
Those looking to enroll in the FLTCIP will soon have to wait a couple of years before applying.
The Office of Personnel Management said it will suspend all new applications to the program starting on Dec. 19. The suspension will last for the next two years, but those who apply ahead of the start date may still see their applications go through. During that time, current FLTCIP enrollees cannot apply to increase their coverage. The suspension will otherwise not affect the coverage of current enrollees.
* * *
The contract for the insurance program, with John Hancock Life and Health Insurance Company, typically lasts seven years before getting a renewal. The program normally gets a premium hike each time the contract turns over. During the open period for new contract proposals earlier this year, only the current underwriter John Hancock submitted a bid. The current FLTCIP contract will expire on April 30, 2023.
The upcoming suspension on applications will allow OPM “to assess the benefit offerings and establish sustainable premium rates that reasonably and equitably reflect the cost of the benefits provided,” the agency said in a Nov. 18 notice. OPM added that it will only suspend applications when it is in the best interest of the program.
Many are eligible to apply for FLTCIP coverage, including federal employees, U.S. Postal Service employees and annuitants, as well as active and retired members of the uniformed services, and qualified relatives of feds. John Hancock has historically sponsored the program, and Long Term Care Partners, LLC, has administered it.
From the Omnicron and siblings front, the National Institutes of Health announced
Reporting a positive or negative test result just became easier through a new website from the National Institutes of Health. MakeMyTestCount.org, developed through NIH’s Rapid Acceleration of Diagnostics (RADx®) Tech program, allows users to anonymously report the results of any brand of at-home COVID-19 test.
COVID-19 testing remains an essential tool as the United States heads into the holiday season and people navigate respiratory viruses. While taking a rapid COVID-19 test has become commonplace, test results are not often reported. COVID-19 test results provide valuable data that public health departments can use to assess the needs and modify the responses in the local community, the state or the nation.
Lab tests have a well-established technology system for sharing test results. RADx Tech has been working on a system to standardize test reporting for at-home tests in a secure manner. The MakeMyTestCount.org website is built on this system for logging test results.
U.S. life insurers paid a record $100 billion in 2021 in death benefits, fueled by another year of Covid-19 deaths, an industry trade group said.
Payouts rose 11% in 2021 to $100.19 billion, most likely due to the pandemic, according to the American Council of Life Insurers. The increase was on the heels of a 15% year-over-year rise in 2020, when death-benefit payments totaled $90.43 billion.
The ACLI compiles data from annual filings by insurers to state insurance departments. Given limitations in the filings, the group can’t break down causes of death, but it is reasonable to attribute the bulk of the increases to the pandemic, said Andrew Melnyk, ACLI vice president of research and chief economist.
The year-over-year increases are among the largest since the 1918 flu pandemic, when payments surged 41%. They are far above the 4.9% average from 2011 to 2021, the ACLI said.
From the No Surprises Act front, Healthcare Dive reports
House lawmakers expressed their discontent with a final rule on surprise billing and urged federal regulators to make changes.
House Ways and Means Committee Chairman Richard Neal, D-Ma., and ranking member Kevin Brady, R-Texas, sent a letter to HHS Secretary Xavier Becerra and other department heads again expressing disappointment with a much-contested section of the surprise billing ban.
The lawmakers “are severely disappointed to find that the August 2022 final rule violates the No Surprises Act in the same ways as before,” Neal and Brady said in a letter last week.
For Heaven’s sake, Congress should give the revised rule a chance before joining the medical associations in condemning it.
From the public health front, Health Payer Intelligence tells us
The number of Americans with a usual source of care has dropped 10 percent in the last 18 years, with only about three-quarters of people saying they have a regular primary care provider or at least a facility where they know they can access care, according to the Primary Care Collaborative (PCC) and AAFP Graham Center.
The analysis also revealed some health disparities, with folks who are Hispanic, have less than a high school education, are uninsured, and are younger being less likely to have a usual source of care than their counterparts. * * *
“Employers have a very important role to play to ensure that all their employees and their families have ready, convenient access to a usual source of affordable primary care,” said Asaf Bitton, MD, the executive director of Ariadne Labs – Harvard T.H. Chan School of Public Health.
“We applaud those employers who are providing highly accessible virtual and in-person primary care options, and working with preferred provider organizations and health systems to support patients in establishing and maintaining these crucial primary care relationships.”
Cardiovascular disease is responsible for about one in five deaths in women in the U.S., more than any other cause — including all forms of cancer combined. Black women like Shields are particularly vulnerable: In the U.S., Black adults are substantially more likely to die from heart disease than their white, Hispanic, or Asian or Pacific Islander counterparts.
To try to reduce deaths from heart disease, health professionals typically use basic risk calculators, which take about a dozen standard data points to predict a person’s likelihood of having a major event, such as a heart attack or stroke, in the next 10 years.
Regardless of their other risk factors, for the most part, patients who are young and female have a very low chance of having a cardiovascular event in the next 10 years, so they are unlikely to get recommendations for serious lifestyle interventions or medication. But they may still be heading down a path to a fatal event later in life.
These data, however, are all missing from standard cardiovascular disease risk calculators. Some pregnancy complications are listed as part of the comprehensive American Heart Association screening guidelines. But a large national 2014 survey revealed that only 16% of primary care physicians and 22% of cardiologists were using these full guidelines. The failure of health-care providers to screen for these sorts of early warning signs is in keeping with the long-standing pattern in which women’s risk for heart disease is chronically underestimated by medical professionals — as well as by women themselves.
That’s a big bowl of wrong.
From the plan design front, Beckers Payer Issues relates
Providers using EHRs that aren’t enabled for electronic prior authorization and the cost to upgrade to those EHRs are the main barriers preventing automated PA, according to a Nov. 14 America’s Health Insurance Plans survey.
The health insurance trade group conducted an industrywide survey on “prior authorization practices and gold carding experience of commercial plans” between February and April, according to the report. AHIP received responses from 26 plans, covering a total of 122 million commercial enrollees.
Top barriers to automated prior authorization:
Provider does not use EHR enabled for electronic PA: 71 percent
Costly/burdensome for providers to buy/upgrade EHR for electronic PA: 71 percent
Lack of interoperability between EHR vendors: 62 percent
Costly for payers to enable PA rules and information to be delivered electronically: 43 percent
Lack of electronic PA solutions on market: 19 percent
This is a surprising outcome considering how vociferously providers object to prior authorization.
The FEHBlog apologizes for the fact that his Grammarly program made a hash out of yesterday’s Miscellany post. The FEHBlog discovered and fixed the problems this afternoon if anyone cares to go back to read that post. Lo siento.
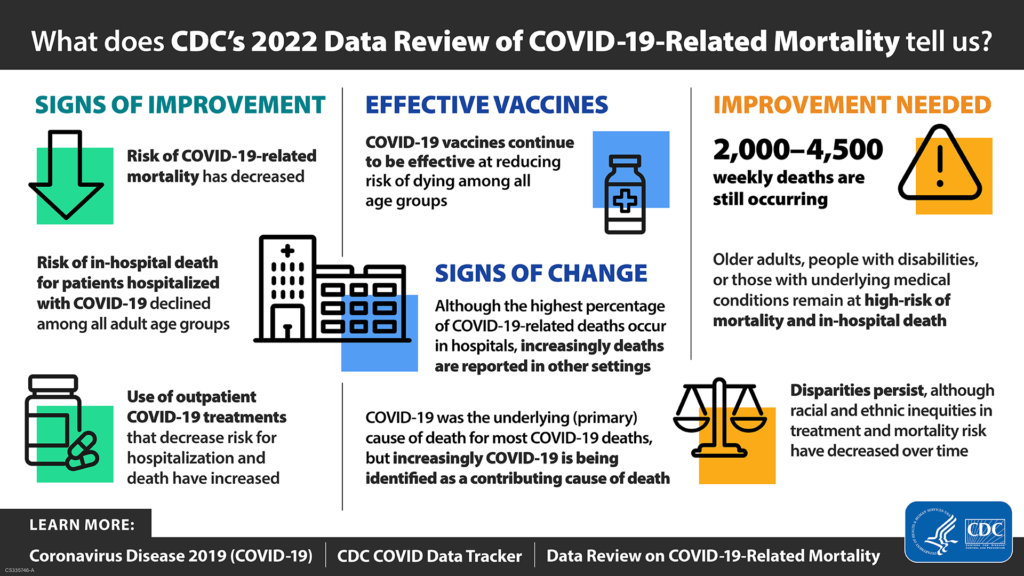
Going forward, the FEHBlog will be posting Covid stats on the first Friday of the month. Here is the CDC’s weekly interpretation of its Covid statistics which focuses on a CDC report on Covid mortality dated November 16, 2022, and summarized below:
Uptake of fall Covid-19 booster shots remains anemic well into November, frustrating public-health experts who blame the lackluster interest on pandemic fatigue and insufficient outreach from officials.
About 31 million people in the U.S. have gotten the updated shots, or roughly 10% of people ages five and older, according to data from the Centers for Disease Control and Prevention. The federal government purchased more than 170 million doses of the new bivalent boosters that target two Omicron subvariants and the original virus strain.
“It has been pretty dismal,” said Rupali Limaye, an associate professor at the Johns Hopkins Bloomberg School of Public Health, who studies vaccine demand and acceptance. * * *
[U]ptake of the modified booster is slow due in part to the limited amount of outreach and type of messaging from health officials, some public-health experts say.
Anecdotally, it sounds like a lot of people are still not aware that the bivalent boosters are available,” said Angela Rasmussen, a virologist at Georgetown University. “If they are, many don’t seem to understand the importance of getting boosted at all—with bivalent or original recipe—and there is a decided lack of urgency in communications about it.”
Some public-health experts say there must be not just more, but also targeted outreach.Celine Gounder, a senior fellow at the Kaiser Family Foundation, said messaging needs to be more targeted at people age 50 and over who are most at risk. Among adults 65 and older, some 27% have gotten an updated booster dose, CDC data show.
“You should be thinking of who is most vulnerable and target the efforts there,” said Dr. Gounder, an infectious-disease specialist and epidemiologist.
The following are the key points from this week’s CDC Fluview:
Seasonal influenza activity is elevated across the country.
The majority of influenza viruses detected this season have been influenza A(H3N2) viruses, but the proportion of subtyped influenza A viruses that are A(H1N1) is increasing slightly.
Two more influenza-associated pediatric deaths were reported this week, for a total of seven pediatric flu deaths reported so far this season.
CDC estimates that, so far this season, there have been at least 4.4 million illnesses, 38,000 hospitalizations, and 2,100 deaths from flu.
The cumulative hospitalization rate in the FluSurv-NET system is higher than the rate observed in week 45 during every previous season since 2010-2011.
The majority of influenza viruses tested are in the same genetic subclade as and antigenically similar to the influenza viruses included in this season’s influenza vaccine.
Medscape offers expert opinions on the “perfect storm” of rampant flu and RSV.
In OPM news, the agency posted its Fiscal Year 2022 Performance and Accountability report this week. The Director’s response to the Inspector General’s list of top management challenges is worth a gander. That response begins on page 125.
From the No Surprises Act front, Beckers Payer Issues tells us
The No Surprises Act has prevented millions of surprise medical bills since January, according to new data from AHIP and the Blue Cross Blue Shield Association.
The payer associations gathered their data, published Nov. 17, by surveying 84 health insurance providers representing around 57 percent of the national market.
“Thanks to the No Surprises Act, millions of Americans no longer face a complicated, confusing billing bureaucracy, being harassed by collection agencies, or even potential legal action,” AHIP President Matt Eyles said in a press release.
AHIP and the BCBS Association also surveyed plans for the number of claims submitted to arbitration under the act. They estimated 275,000 claims have been submitted since January 2022, more than the 17,000 claims predicted by government agencies.
AHIP is backing HHS in a lawsuit over surprise billing arbitration from Texas providers, who have support from the largest associations of providers.
The trade association filed an amicus brief in Texas Medical Association v. HHS on Nov. 16.
The lawsuit, filed by the Texas Medical Association in September, challenges the arbitration process established under the No Surprises Act.
The FEHBlog appreciates AHIP’s amicus brief filing. In the FEHBlog’s opinion, the medical association plaintiffs in the Texas case are making a mountain out of a molehill.
A surprising legal development was the Justice Department’s 11th hour notice of appeal filed today in the antitrust challenge to United Healthcare’s acquisition of Change Healthcare which a federal district judge approved last September.
The emergence of interchangeable biosimilars since the pathway opened up has been slow. But the FDA on Thursday approved the fourth interchangeable biosimilar, which is also the second interchangeable biosimilar insulin product.
Eli Lilly’s Rezvoglar (insulin glargine-aglr), which converted to an interchangeable after an earlier biosimilar approval in December 2021, follows Viatris’ Semglee in seeking out a niche to compete with Sanofi’s blockbuster Lantus (insulin glargine). * * *
These interchangeable designations mean Semglee and Rezvoglar may be substituted at the pharmacy level for Lantus, without a doctor’s prescription, and as long as the state pharmacy law permits the switch.
Preterm births last year reached their highest peak since 2007 – with more than 383,000 born before 37 weeks of gestational age in the United States, according to a new report.
Of all groups, Asian and Pacific Islander mothers saw the largest preterm birth increase – an 8% surge – even though births to Asian mothers decreased that year, and they have the lowest preterm birth rate overall.
HHS’s Agency for Healthcare Quality and Research capped off antibiotic awareness week by releasing antibiotic stewardship kits for the acute hospital, long-term care, and ambulatory care settings.
From Capitol Hill, the Wall Street Journal reports
Republicans won a majority of seats in the House of Representatives with a victory in California, the Associated Press said late Wednesday, bolstering their ability to steer the agenda on Capitol Hill after two years of Democratic control of both chambers of Congress and the White House.
The Congressional Research Service released a report on health care provisions expiring at the end of this 117th Congress.
With midterm elections resulting in a narrowly divided Congress, the HHS will be free to focus on longstanding priorities for the health department, such as implementing drug negotiation policy within Medicare, HHS Secretary Xavier Becerra said at the HLTH conference in Las Vegas on Tuesday.
“In a way, we’re now going to be able to concentrate on the work we have to still execute on,” Becerra said,
Under the Inflation Reduction Act passed earlier this year, Congress granted Medicare the power to negotiate how much it pays for certain prescription drugs starting in 2026, and to receive rebates from pharmaceutical manufacturers that hike drug costs above the rate of inflation starting in 2023.
Of course, HHS and its partners have a lot of work on implementing the No Surprises Act. Health Payer Intelligence discusses the good faith estimate and advance explanation of benefits comments that an ERISA plan trade association, ERIC, submitted to the NSA regulators yesterday.
In other HLTH 2022 conference news,
Healthcare Dive tells us about Google’s plans for offering personal health records and Maven Clinic‘s efforts to build a maternal health business by, e.g., recently landing a $90 million Series E amid increasing investor focus on women’s health.
MedCity News informs us, “Cell and gene therapies are offering patients potentially curative treatments for a growing scope of diseases. Insurance companies are trying to figure out how to pay for them. Industry consultants speaking at the HLTH conference offered some strategies they see payers taking to these new therapies.”
From the federal employee benefits front,
Govexec collected all of its current Open Season articles for convenient access.
Reg Jones, writing in Fedweek, recommends that federal employees contemplating retirement should retire on December 31, 2022.
Govexec reports that the Postal Service is headed into its busy season with far fewer employees than past years.
From the Affordable Care Act front —
The FEHBlog ran across this updated reference chart on minimum essential coverage under the ACA.
The U.S. Preventive Services Task Force issued its 12th Annual Report to Congress which is titled “High-Priority Evidence Gaps for Clinical Preventive Services.”
From the public health front —
Forbes reports “Researchers at the University of Houston have developed a vaccine that could block the effects of fentanyl and prevent addiction, according to a new study that could unlock solutions to the opioid epidemic as more than 150 people die every day from overdoses connected to synthetic opioids.”
CNN reports “The five-year lung cancer survival rate has increased 21%, from 21% in 2014 to 25% in 2018, making what experts call “remarkable progress” – but it is still the leading cause of cancer death in the United States. However, in communities of color, a person’s odds of surviving five years after diagnosis are much lower, at only 20%, according to the 2022 State of Lung Cancer report, which was published by the American Lung Association on Tuesday.”
The National Institutes of Health tells us “COVID-19 Vaccines Are Safe for People Receiving Cancer Immunotherapy, Study Confirms.”
From the miscellany department —
Forbes informs us “UnitedHealth Group’s pharmacy benefit manager Optum Rx Tuesday said it will put three less expensive “biosimilar” versions of Abbvie’s pricey rheumatoid arthritis drug Humira ‘in the same position as the brand’ on the PBM’s preferred list of drugs known as a formulary.”
Over 200 members of the Senior Executive Service this year will receive Presidential Rank Awards, considered the highest honor for career civil servants.
President Joe Biden picked 233 winners across a total of 33 different agencies for the 2022 awards program, the Office of Personnel Management announced on Nov. 15.
“Each and every day, our federal employees are working to address the nation’s most pressing issues, developing technologies to improve millions of lives, and ultimately, achieving the seemingly unachievable on behalf of the American public,” OPM Director Kiran Ahuja said in a press statement. “This year’s Presidential Rank Awards reflect the Biden-Harris administration’s support for hardworking civil servants who exemplify strength, integrity, industry and a relentless commitment to public service through their exceptional leadership, contributions and accomplishments.”
Kudos to the winners.
From the Omicron and siblings front, the Wall Street Journal reports
Moderna Inc.’s new updated Covid-19 booster shot for the U.S. generated strong immune responses in people against Omicron subvariants, according to the first data from a company-sponsored study testing the new doses in volunteers.
Moderna said Monday that people receiving the updated booster shot had more than five times the neutralizing antibodies against Omicron subvariants BA.4 and BA.5 than people who received Moderna’s original booster shot, which targeted an earlier strain of the coronavirus.
“That really bodes well for the vaccine and public health,” Moderna President Stephen Hoge said in an interview.
From the conferences’ front —
The American Medical Association explains what happened on the closing day of the AMA’s interim meeting.
Healthcare Dive offers Dive Briefs from the HLTH conference about Included Health and Elevance Health. Fierce Healthcare adds “Mental health provider SonderMind acquired neuroscience company Total Brain with the goal of revolutionizing personalized therapeutic care and providing individual insights into mental wellbeing.”
“Amazon has launched a message-based virtual health service called Amazon Clinic a little more than two months after the retail giant shuttered its primary care delivery business Amazon Care.
“Amazon Clinic, which is currently live and available 24/7 through Amazon’s website and mobile app, is a marketplace for telemedicine providers, connecting consumers with virtual doctors who can diagnose, treat and prescribe medication for a range of common health conditions like acne, birth control and migraines, the retail giant said.
“Amazon Clinic will be available in 32 states at launch, with plans to expand to additional states in the coming months, according to a Tuesday blog post announcing the news. * * *
“Consultation cost will vary by provider, including follow-up messages with a clinician for up to two weeks after the consultation. Consultations start at $30.
“Amazon Clinic does not accept insurance. The company didn’t disclose whether that would change in the future.”
Nearly a decade after unsuccessfully attempting a merger, South Dakota-based Sanford Health and Minnesota’s Fairview Health Services said Tuesday they’re again in talks to combine.
The two regional health care giants say they intend to complete a merger next year. The new entity would be called Sanford Health and be run by Sanford’s current CEO. The deal would include the University of Minnesota hospitals, which Fairview purchased in 1997.
Financial details and any cost-cutting plans tied to the proposed merger were not immediately disclosed.
From the Food and Drug Administration front —
On Thursday [November 10], the FDA, in conjunction with the CDC, released results on youth tobacco use from the 2022 National Youth Tobacco Survey. Findings show that in 2022, more than one in 10 middle and high school students (3.08 million) had used a tobacco product during the past 30 days – including 16.5% of high school and 4.5% of middle school students. The full results are available here.
Today, the FDA announced an unprecedented advancement in foodborne illness prevention through the finalization of a rule to more effectively trace contaminated food through the food supply, whether sourced in the U.S. or abroad.
Also [t]oday, the FDA issued a Federal Register notice, Safety and Effectiveness of Certain Naloxone Hydrochloride Drug Products for Nonprescription Use, that may help facilitate the development and approval of certain nonprescription naloxone drug products, including through the switch of certain naloxone drug products from prescription status to nonprescription status. Naloxone is a medicine that can help reduce opioid overdose deaths and when administered timely, usually within minutes of the first signs of an opioid overdose, can counter the overdose effects.
From the No Surprises Act front, today was the deadline for the public to submit comments to the NSA regulators concerning two unnecessarily complicated consumer protections found in the law — the good faith estimate and the advance explanation of benefits. In the FEHBlog’s view, the NSA regulators would be well served if they limited those protections to surprise billing situations not elsewhere covered by the law, for example, (1) complicated procedures and (2) reoccurring services that take place over a prolonged period, e.g. chiropractor care, mental health care. The WEDI group, which is an advisor to the HHS Secretary, also offers useful comments on the matter.
From the Affordable Care Act front, the U.S. Preventive Services Task Force gave an inconclusive (I) grade today to screening for obstructive sleep apnea in adults. “The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for obstructive sleep apnea in the general adult population.” The USPSTF previously graded the apnea screening service an I grade in January 2017.
The Earth is now home to eight billion people, the United Nations said, because people are living longer and fertility rates have surged in some countries. * * *
There were about 300 million people on Earth two millennia ago, according to the U.N. The population fluctuated in the centuries after that, largely because of plagues and natural disasters. Then the population accelerated, reaching one billion in 1804, four billion in 1974 and seven billion in 2011. * * *
Demographers project the world will reach its next population milestone—nine billion—around 2037.
The U.N. predicts that the global population will peak at around 10.4 billion during the 2080s and remain near that level until the start of the next century. Another forecast, from the Wittgenstein Centre for Demography and Global Human Capital at the University of Vienna, has it peaking at 9.67 billion in 2070, before a slow decline as fertility rates drop.
the Novavax COVID-19 Vaccine, Adjuvanted (NVX-CoV2373) has received emergency use authorization (EUA) from the U.S. Food and Drug Administration (FDA) to provide a first booster dose at least six months after completion of primary vaccination with an authorized or approved COVID-19 vaccine to individuals 18 years of age and older for whom an FDA-authorized mRNA bivalent COVID-19 booster vaccine is not accessible or clinically appropriate, and to individuals 18 years of age and older who elect to receive the Novavax COVID-19 Vaccine, Adjuvanted because they would otherwise not receive a booster dose of a COVID-19 vaccine.
“The U.S. now has access to the Novavax COVID-19 Vaccine, Adjuvanted, the first protein-based option, as a booster,” said Stanley C. Erck, President and Chief Executive Officer, Novavax. “According to CDC data, almost 50 percent of adults who received their primary series have yet to receive their first booster dose. Offering another vaccine choice may help increase COVID-19 booster vaccination rates for these adults.”
Moderna Inc said on Wednesday its COVID-19 vaccine booster targeting the BA.1 subvariant of Omicron generated a strong immune response against that variant, with antibody levels staying high for at least three months.
Omicron-tailored shots by Pfizer Inc and Moderna are already authorized by regulators in several countries. The United States has given the go-ahead for booster vaccines that target the currently circulating BA.4 and BA.5 subvariants of Omicron.
The New York Times provides an update on the new Omicron variants, including this critical point
Fortunately, Paxlovid works against these new variants. The mutations that make them spread so quickly are changes to the surface of the virus where it locks onto cells and where antibodies attach to it. Paxlovid attacks the virus in a different way. It detects the virus after it’s inside the cell and is replicating, and these new subvariants seem to be just as vulnerable to Paxlovid as the earlier variants.
Federal funding was crucial in enhancing access to coronavirus resources during the initial phases of the pandemic, but questions remain about what will occur when the public health emergency ends and how it will impact consumer healthcare spending, according to a Kaiser Family Foundation brief.
The end of the public health emergency is still undetermined. However, experts have projected that it will end in 2023. The scheduled termination has been pushed back multiple times. Its final termination will signal the end of various flexibilities and protections that have been tied to the declaration.
Additional Covid funding is likely to occur in the Congressional lame-duck session following the November 8 election, in the FEHBlog’s opinion.
Patient volumes continue to remain below pre-pandemic levels for hospitals and health systems this year as COVID-19 likely accelerated a shift to outpatient settings, a new report finds.
Consulting firm Kaufman Hall released its “2022 Healthcare Performance Improvement” report (PDF), which outlines the barriers hospitals and health systems face in a rough year financially. Another key obstacle continues to be workforce shortages, as more and more facilities shift resources to retain staff.
“Healthcare leaders must navigate short-term challenges that continue to pressure revenue and expenses, while also adapting organizational strategy to match larger transformations in the way care is delivered,” said Kaufman Hall Managing Director Lance Robinson in a statement on the report.
and offers a discussion of an expert-touted hybrid approach to compensating primary care providers. In the FEHBlog’s view, adequately paying PCPs is critically important to resolving SDOH and mental health issues adversely impacting our country.
In the regard
A National Institutes of Health study uncovered racial disparities in advanced cardiac care.
When Sarka Lisonkova and her colleagues set out to study disparities in the birth outcomes of people who’ve used methods like IVF, they figured that any inequities that existed would be narrower in this group. After all, it can be expensive to get pregnant with medical assistance, and wealth is tied to better outcomes.
Instead, the researchers reported Wednesday, the racial and ethnic disparities for some metrics were even wider for babies of parents who had used IVF or other fertility treatments than among children who were conceived “spontaneously.”
One key finding: while neonatal mortality rates were twice as high among spontaneously conceived children of Black women versus white women, they were four times as high among infants of Black women conceived through technologies like IVF, according to the researchers’ study, which was published in the journal Pediatrics.
The National Committee for Quality Assurance gives us an update on their efforts to stratify HEDIS measures results by racial and ethnic categories.
In other U.S. healthcare business news, Healthcare Dive reports
As the U.S. heads toward a possible recession, Elevance Health CEO Gail Boudreaux said the insurer is preparing for a possible economic decline.
“Certainly we’re mindful of an economic downturn. We’re planning for it in our businesses,” Boudreaux said on a Wednesday call with investors to discuss third-quarter earnings.
Elevance’s profit climbed to $1.6 billion for the third quarter, a 7% increase compared with the prior-year period on a bigger membership base of 47.3 million members.
Despite little growth in the cost of medical services over the last year, inflation has finally caught up with healthcare.
As of September, medical services costs have risen 6.5 percent year over year, according to a Bureau of Labor Statistics report released Oct. 13.
Analysts like Fitch have said the rise in costs will lead to payers raising insurance premiums across the board because of the growing cost pressures on providers, including workforce disruptions.
Studies have already confirmed employers are preparing for higher healthcare expenditures next year because of inflation. Aon analysts said Aug. 18 that U.S. employers’ healthcare costs are expected to rise by an average of 6.5 percent, or $13,800 per employee, in 2023.
“The only 100 percent sure way to keep within budget as the medical industry (especially hospitals) demand more and more is to raise premiums, increase deductibles, higher copays and coinsurance,” James Gelfand, president of the ERISA Industry Committee, told The Washington Post Oct. 14. “Employers hate to do this, but the medical-industrial complex demands an ever-increasing share of workers’ wages.”
The rise in insurance costs could begin to appear when employees sign up for employer-sponsored coverage during their next enrollment period, a trend that could continue through at least 2024, according to the Post.
A large commercial insurer’s decision to cover a controversial class of software-based treatments for psychiatric and other conditions could prove to be a landmark moment in the development of these so-called prescription digital therapeutics, which until now had been unable to secure coverage from insurers skeptical that the new technologies are as effective as their makers claim.
Pittsburgh-based Highmark quietly put in place a policy in August describing when these treatments may be “medically necessary,” which paves the way for the health insurer to be the first to cover the category for a population of millions of members.
The policy indicates Highmark’s intention to pay for claims only for prescription digital therapeutics cleared by the Food and Drug Administration when prescribed by a clinician within the appropriate specialty and used as indicated on product labels. Highmark is currently negotiating with product developers about how much it will pay for individual treatments and over details such as what constitutes an “episode of care,” said Matt Fickie, a senior director at Highmark, which has 6 million members in Pennsylvania, Delaware, West Virginia, and New York. “That’s the part that is sticky and that requires additional work,” he told STAT.
After an extraordinary three-day hearing, an expert panel of advisers to the U.S. Food and Drug Administration voted on Wednesday to uphold an effort by the regulator to withdraw a controversial drug for preventing premature births.
The 14-to-1 vote came after the agency and Covis Pharma, the manufacturer of the drug, offered highly contrasting views of reams of clinical evidence — which they parsed in excruciating detail — in order to settle the fate of the treatment, known as Makena.
The FDA successfully persuaded the panel that the medication should be withdrawn because the results of a clinical trial, which was required when the agency approved Makena [on an accelerated basis] in 2011, failed to show the expected benefit. For its part, Clovis maintained that a follow-up trial showed its drug did benefit a select subset of patients — including Black women — but struggled to convince the panel that the drug should remain available while a lengthy follow-up study is run to confirm its argument.
The sentiment among most panelists was reflected in remarks by Susan Ellenberg, a professor emeritus of biostatistics, medical ethics, and health policy at the Perelman School of Medicine at the University of Pennsylvania, who said “unmet need is not a basis for keeping a drug available when you don’t know if it works.”
The FDA Commissioner, Robert Califf, MD, is the final decision maker.
The NCQA has created
A new website adds two key resources in the fight against antibiotic resistance:
* A How-To Toolkit: Webinars and written summaries outline best practices, emerging trends and lessons from the field about savvy stewardship of antibiotics.
* An “Honor Roll”: Learn which health plans’ management of antibiotics leads the industry.
From the No Surprises Act front, CMS today issued updated guidance on how to initiate an NSA arbitration. The new guidance reflects the revised final independent dispute resolution rule published this past summer.
From the FEHB Open Season front, OPM issued today its annual open season benefits administration letter identifying FEHB and FEDVIP contract changes for 2023 A/K/A, the Significant Changes letter and appendix. OPM also released its Federal Benefits Fast Facts for the upcoming Open Season.
From the No Surprises Act front, Newfront, an insurance brokerage, issued an important reminder on the revised NSA consumer notice that health plans must post by January 1, 2023. Here are the current and future notices.
From the Covid vaccine mandate front, the Miller & Chevalier law firm tells us
On October 14, 2022, the Safer Federal Workforce Task Force released a roadmap for federal contractors of anticipated guidance on how federal agencies would be handling the implementation and enforcement of the federal contractor vaccine mandate and workplace safety requirements of Executive Order 14042, “Ensuring Adequate Safety Protocols for Federal Contractors.” The Task Force — created by President Biden to provide guidance to federal agencies on handling operational issues related to the COVID-19 pandemic — anticipates a “potential narrowing of the existing nationwide injunction on October 18, 2022.” As a result, the Task Force anticipates the release of three documents: (1) notice from the Office of Management and Budget (OMB) to federal agencies regarding compliance with injunctions and the inclusion of vaccine mandate clauses in future solicitations and contracts; (2) updates to Task Force guidance on safety protocols for covered contractor and subcontractor workplace locations, including a timeline for implementation; and (3) additional guidance from OMB on “timing and considerations for provision of written notice from agencies to contractors regarding enforcement of contract clauses” implementing vaccine and workplace safety mandates. Notably, until OMB issues the guidance above, agencies are directed not to take any steps to require compliance with the Task Force guidance or enforce any contract clauses implementing the requirements of Executive Order 14042.
This Task Force guidance stems from an August 26, 2022, U.S. Court of Appeals for the 11th Circuit opinion replacing the lower court’s nationwide injunction with an injunction applying to the plaintiffs. However, several other U.S. Courts of Appeals are hearing cases involving this mandate so we may be waiting a while for the OMB guidance.
Also, from the Omicron and siblings front, Beckers Hospital Review discusses the new Omicron variants BQ.1 and BQ1.1.
CDC estimates indicate a new omicron variant, BQ.1, and its descendent BQ.1.1 account for 11.4 percent of cases nationwide. The pair have been dubbed “escape variants” for their ability to escape immunity and are currently most prevalent in New York and New Jersey, where they account for nearly 20 percent of new infections. * * *
Experts are optimistic that the bivalent omicron boosters will offer protection against BQ.1 and BQ.1.1 since they’re descendants of BA.5. (Updated boosters are designed to target the original SARS-CoV-2 strain, BA.4 and BA.5.)
“The bad news is that there’s a new variant that’s emerging and that has qualities or characteristics that could evade some of the interventions we have. But, the somewhat encouraging news is that it’s a BA.5 sublineage, so there are almost certainly going to be some cross protection that you can boost up,” Dr. Fauci said.
From the monkeypox front, the American Hospital Association reports
The Centers for Disease Control and Prevention today reported the first U.S. monkeypox case in a health care worker since the outbreak began in May. The report describes how an emergency department nurse in Florida was exposed to the virus through a needlestick, and recommends approaches to preventing infections in health care workers. CDC also released a report describing five patients who acquired ocular monkeypox, a rare but sight-threatening condition, including four who were hospitalized. The report recommends health care providers advise monkeypox patients to practice hand hygiene and avoid touching their eyes, and consider urgent ophthalmologic evaluation and monkeypox-directed treatment for patients with ocular signs and symptoms.
The U.S. is seeing flu activity rise earlier than usual, with Southern states reporting the highest levels of activity, according to the CDC’s latest FluView report for the week ending Oct. 8.
Overall, activity remains low, “but increasing in most of the country,” the CDC said. HHS region 4 (Kentucky, Tennessee, Mississippi, Alabama, Georgia, South Carolina, North Carolina, Florida) and region 6 (New Mexico, Texas, Oklahoma, Arkansas, Louisiana) are reporting the highest levels of flu activity.
Furthermore, STAT News “talked on Friday with Lynnette Brammer, a flu epidemiologist and team lead for domestic surveillance in the CDC’s influenza division, to get a sense of what the agency is seeing.”
Thinking about this flu season and what you’re seeing so far, what’s your best guess for what’s ahead?
Our syndromic surveillance methods are much trickier to try and interpret now, with Covid in the picture. It just muddies the water, basically.
We’ll have to see if the flu and Covid circulate at the same time. Right now, it looks like Covid is still trending down in a lot of the country, but flu’s going up in a lot of the country.
If individuals start to feel crappy this winter, how will they know if it’s a cold? Flu? Covid?
I think testing is going to be really important given that, for flu and Covid, there are treatments that — particularly for high-risk people — can make a huge difference in how well they are able to get through their illness. So it’s going to be really important to test so physicians can know the appropriate treatment for their patients.
In related news, the Government Accountability Office released a report on routine vaccination rates in our country.
U.S. school children generally have higher rates of vaccination to protect them from preventable illness compared with adults.
We found gaps in adult rates for flu, shingles, tetanus, and pneumococcal (prevents pneumonia and more) vaccines. Among other things:
Adults were about 40% more likely to get the tetanus and pneumococcal vaccines than the shingles vaccine
Vaccination rates for Black or African American and Hispanic or Latino adults were about 13% below that of White adults for each vaccine
Health and Human Services is using social media and its website to raise public awareness on the importance of being vaccinated.
From the ACA reporting front, the Internal Revenue Service issued its Forms 1095-B and 1095-C for 2022. The Service also released an employee fringe benefits guide for federal, state, and local government employers.
From the Rx coverage front, BioPharma Dive predicts “five questions facing drugmakers as third-quarter earnings begin. Alzheimer’s study results, drug pricing law, bring new questions for many of the industry’s top companies.”
From Capitol Hill, the Wall Street Journal reports
Sen. Joe Manchin (D., W.Va..) on Tuesday threw in the towel on including his contentious proposal to speed up permitting of energy projects in a must-pass funding bill, clearing the way for the Senate to advance the legislation needed to keep the government open.
With the permitting language out, the Senate voted 72 to 23 to advance the stopgap bill, which would extend current government funding levels until Dec. 16 and prevent a partial shutdown this weekend, when the fiscal year ends. The bill now moves to final passage in the Senate and will also need approval in the House, which returns Wednesday, before heading to President Biden’s desk. * * *
The resolution would also reauthorize the Food and Drug Administration’s user-fee agreements for prescription drugs, generic drugs and medical devices, preserving their access to U.S. patients. The legislation has to pass by the end of September to avoid funding gaps for the FDA.
From the monkeypox front, STAT News reports that responding to the disease is stretching thin the resources of public health clinics serving the LGBTQ+ communities.
Today was filled with surprises.
The Centers for Medicare and Medicaid Services beat OPM to the punch by announcing 2023 Medicare Part B premiums before OPM announced 2023 FEHB and FEDVIP premiums. “The standard monthly premium for Medicare Part B enrollees will be $164.90 for 2023, a decrease of $5.20 from $170.10 in 2022. The annual deductible for all Medicare Part B beneficiaries is $226 in 2023, a decrease of $7 from the annual deductible of $233 in 2022.”
BioPharma Dive reports “In a surprise result, Alzheimer’s drug from Eisai and Biogen shows benefit in a large trial; The drug, called lecanemab, met the study’s main and secondary goals, reducing clinical decline [by 27%] over 18 months compared to a placebo.” The announcement’s timing is exquisite because, for 2022, CMS jacked up the Medicare premiums in anticipation of massive costs from what turned out to be a failed Alzheimer’s drug, Aduhelm, also from Biogen. The popping of the Aduhelm balloon resulted in the Medicare Part B premium and deductible decreases for 2023. FEHB carriers need to keep an eye on this drug’s progress because FEHB plans have large cadres of annuitants with Part A but not Part B due to IRMAA.
From the No Surprises Act front, the American Hospital Association reports
The AHA, American Medical Association and Medical Group Management Association today urged the Centers for Medicare & Medicaid Services not to include a convening/co-provider framework when implementing the Advanced Explanation of Benefits and insured good faith estimate provisions under the No Surprises Act. The groups urged the agency to instead allow each billing provider to submit their own good faith estimate to the health plan to create an AEOB; and to leverage existing provider and health plan workflows, standards and technologies for claim submission and adjudication to support accurate AEOBs for patients.
“Our organizations appreciate the opportunity to work with CMS on the No Surprises Act’s price transparency provisions implementation, and we are committed to working closely with our members to ensure that they have the information and tools to successfully implement the new requirements,” the letter adds. “Additionally, we remain committed to ensuring that patients have access to complete and accurate out-of-pocket cost information for scheduled care and working with you to develop efficient methods of delivering this information.”
This sensible idea would align the GFI with regular EOBs, thereby facilitating the use of electronic claims technology.
From the benefit design front, Fierce Healthcare reports
Walmart, the largest employer in the U.S., is teaming up with fertility startup Kindbody to offer benefits under its insurance plan that will help its workers expand their families.
Walmart Associates and their dependents who are enrolled in a self-insured Walmart medical plan will now have access to Kindbody’s services including fertility assessments and education, fertility preservation, genetic testing, in vitro fertilization (IVF) and intrauterine insemination (IUI).
Walmart’s employees will have access to more than 30 state-of-the-art Kindbody clinics across the U.S., including a new clinic and IVF lab in Rogers, Arkansas that will provide comprehensive virtual, at-home and in-clinic care. The new facility is expected to open later this year.
The expanded services build on Walmart’s Center of Excellence (COE) model, which provides benefit support and coverage for certain heart, spine and joint surgeries and cancer treatments.
“Providing access to high-quality health care is very important to us, and we’ve heard from our associates that improved access to fertility, surrogacy and adoption support is a priority for them and their families,” said Kim Lupo, senior vice president, Walmart Global Total Rewards in a statement. “Through Kindbody, Walmart associates in every corner of the country will have access to a variety of services to aid in their family-planning journey.
From the studies/research department
Beckers Payer Issues informs us, “Alabama, Hawaii, Florida, New York and New Jersey are the states with the highest incidences of low-value care, a new study published in Health Affairs found.”
The National Institutes of Health (NIH) announced “a new program to better understand the function of every human gene and generate a catalog of the molecular and cellular consequences of inactivating each gene. The Molecular Phenotypes of Null Alleles in Cells (MorPhiC) program, managed by the National Human Genome Research Institute, aims to systematically investigate the function of each gene through multiple phases that will each build upon the work of the previous.” Wow.
NIH also tells us, “People with opioid use disorder who received telehealth services during the COVID-19 pandemic were more likely to stay on their medications and less likely to overdose. The findings support continuing the expanded telehealth access that began during the pandemic.”
From the tidbits department
The US Preventive Services Task Force today reaffirmed an A grade recommendation for screening for syphilis infection in asymptomatic, nonpregnant adolescents and adults who are at increased risk for infection. The initial recommendation for this screening was made in 2016.
Beckers Health IT explores the significant business benefits of United Healthcare’s recent antitrust litigation victory, which allows UHC’s acquisition of change healthcare to proceed.
The American Hospital Association, along with a coalition of other healthcare organizations, wants the HHS to postpone an information blocking deadline slated to start Oct. 6, according to a Monday letter sent to Secretary Xavier Becerra.
By that date, providers, health IT developers and others must start sharing all electronic protected health information in a designated record,effectively prohibiting entities from information blocking.
The groups warn they’re not prepared to meet the deadline and are struggling to interpret a clear definition of electronic health information or technical infrastructure to support secure exchanges, according to the release.
Yesterday, the FEHBlog welcomed the first day of autumn when the autumnal equinox was at 9:04 pm today. To compound his error, the FEHBlog overlooked that yesterday was World Gratitude Day. The FEHBlog is grateful for his readers.
From Capitol Hill, Roll Call reports on the state of the continuing resolution to fund the federal government into mid-December.
Congressional leaders and appropriators are expected to spend the weekend haggling over the last details of the text Schumer is aiming to unveil Tuesday [following the Jewish New Year holiday], which he would offer as a substitute amendment.
On Thursday, authorizing committees agreed on a five-year reauthorization of FDA user fee programs, which could potentially be attached to the continuing resolution. Numerous other authorizations, funding “anomalies” and a supplemental aid package for Ukraine and other purposes were still being negotiated.
The House of Representatives is capable of acting quickly.
From the Omicron and siblings’ front
Beckers Hospital Review reports, “Retooled COVID-19 booster shots that target omicron subvariants could be authorized and available for children to receive within a month, the CDC said in a vaccination planning guide released Sept. 20.”
The Wall Street Journal informs us, “Since the new boosters became available [for people 12 and older] earlier this month at pharmacies, doctors’ offices and elsewhere, about 4.4 million people have received a new booster shot, the Centers for Disease Control and Prevention said Thursday.”
In other public health news, STAT News tells us
As some of us wonder how we’ll know when the coronavirus pandemic is over, a new report from the WHO called “Invisible Numbers” reminds us that noncommunicable diseases take more lives than infectious diseases (and make Covid-19 worse). To wit: Cardiovascular diseases including heart disease and stroke, cancer, diabetes, chronic respiratory diseases, and mental illness cause nearly three-quarters of deaths in the world and kill 41 million people every year. Some of the more striking findings:
* Every year 17 million people under age 70 die of noncommunicable diseases, 86% of whom live in low- or middle-income countries.
* Preventable risk factors include tobacco use, unhealthy diets, harmful use of alcohol, physical inactivity, and air pollution.
* NCDs cause 74% of all deaths, but interventions known to work could avert at least 39 million NCD deaths by 2030.
Cancer deaths in the United States are continuing to decline, according to a new report from the American Association for Cancer Research.
The report, published Wednesday, found that deaths from cancer have decreased by 2.3% every year between 2016 and 2019.
Overall, there has been a 32% reduction in the U.S. cancer death rate since 1991, which translates into approximately 3.5 million lives being saved, the report said.
Additionally, in 2022, there are more than 18 million cancer survivors living in the U.S., equivalent to 5.4% of the population, the report found. Fifty years earlier, there were just 3 million cancer survivors.
New results from a large prospective trial give a better idea of how a blood test that can detect multiple cancers performs in a “real-life” setting.
“As this technology develops, people must continue with their standard cancer screening, but this is a glimpse of what the future may hold,” commented study investigator Deborah Schrag, MD, MPH, chair, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York City.
The National Institutes of Health on Thursday announced more than $600 million in fresh funding for an expansive and ongoing push to unravel the mysteries of the human brain, bankrolling efforts to create a detailed map of the whole brain, and devise new ways to target therapeutics and other molecules to specific brain cell populations.
Scientists across the country are involved, from teams at the Salk Institute to Duke University to the Broad Institute of MIT and Harvard, among other places. If successful, they will help answer fundamental questions about the body’s most complex organ. What are all the cell types in the brain? How are they connected to one another? How do the workings of the brain change during disease, and what can we do about that?
So far, those questions have proven easier to ask than to answer, with researchers gleaning bits of information from individual studies, but the hope is that a broad-based effort will jump-start new revelations.
CVS Health is making progress toward its behavioral health goal of decreasing the suicide rate among Aetna members by 20 percent by 2025, but progress among adolescent members is lagging, the healthcare organization announced.
“Our members are not immune to the national suicide crisis reported by the CDC. Though we are on track lowering suicide attempts in adults, our goal will not be reached until we can say the same for adolescents,” said Sree Chaguturu, MD, executive vice president and chief medical officer at CVS Health.
The organization has been working toward this goal since 2017, its work running parallel to that of the American Foundation for Suicide Prevention (AFSP) which had the same goal.
As of March 2022, CVS Health saw suicide attempts among Aetna members drop by 15.7 percent when compared to the company’s 2019 rate.
CVS Health broke down the overall rate by age and found that the reductions were largely driven by decreases among members ages 18 and older. For individuals in this age range, suicide attempts dropped by 17.5 percent in 2021 and dropped another 34.1 percent through March 2022.
Having made progress toward the goal, however, the organization does not intend to slow down.
“We are doubling down on efforts to prevent suicide in teens by identifying those most at-risk and in need of intervention, reaching out to those discharged from the ER after a suicide attempt with resources and supporting parents and loved ones in prioritizing the mental health of their kids,” Chaguturu explained.
Specifically, Aetna saw an upward trend in suicide attempts among its adolescent members.
Members between the ages of 13 and 17 saw increases in suicide attempts. In 2021, the suicide rate among this population grew 43 percent. In the first three months of 2022, the suicide rate jumped another 32 percent.
“We are implementing evidence-based therapies and outreach programs to prevent suicidal ideation before it starts and get adolescents the clinical care they need when they are at risk,” said Cara McNulty, president of behavioral health and mental well-being at CVS Health. “Every suicide attempt prevented, life saved, and mental health resource sought is an important step to reducing death by suicide in the United States.”
Mazaal Tov to CVS Health for those successful and ongoing efforts.
The Society for Human Resources offers guidance on suicide prevention in the workplace.
From the No Surprises Act litigation front, STAT News explains
During a hearing yesterday, the Association of Air Medical Services indicated it was following in the footsteps of AHA and AMA and would likewise dismiss its claims now that the final rules are out. But the AAMS also said it was deliberating whether it would file a different lawsuit in a different court, while attorneys for AMA and AHA backpedaled and said they have no intentions of filing any new lawsuits anywhere.
Today we got some clarity when the Texas Medical Association filed a new lawsuit challenging the revised final independent dispute resolution rule issued in the summer. In addition, the American Hospital Association and the American Medical Association have announced that they are joining the case as friends of the court in support of the Texas Medical Association. The lawsuit was filed in the U.S. District Court for the Eastern District of Texas. And the beat goes on.
From the U.S. healthcare business front, the Wall Street Journal reports
The talks are serious and a deal to purchase Cano could be struck in the next several weeks, assuming the negotiations don’t fall apart, some of the people said. Cano shares, which had been down nearly 7%, turned positive and closed up 32% after The Wall Street Journal reported on the talks with Humana and other unnamed parties, giving the company a market value of roughly $4 billion.
Bloomberg subsequently reported CVS’s interest.
It couldn’t be learned which other potential buyers might be in the mix, but Cano could be Humana’s to lose as the health insurer has a right of first refusal on any sale, part of an agreement that was originally struck in 2019.
Miami-based Cano operates primary-care centers in California, Florida, Nevada, New Mexico, Texas, Illinois, New York, New Jersey and Puerto Rico, according to documentation from the company. It mainly serves Medicare Advantage members, a private-sector alternative to Medicare for seniors.
Healthcare startup Curative, best-known for providing COVID-19 testing, is introducing a health plan with no copays or deductibles.
The company is offering the new plan in the Austin, Texas, area, with plans to expand throughout Texas over the next year, Curative said Sept. 21. The announcement comes as the startup lays off 109 employees from its testing business in California.
In a news release, Fred Turner, co-founder and CEO of Curative, said the startup is on a mission to “drastically remake” the U.S. healthcare system.
“The only way to achieve true cost transparency is for all in-network services to be covered at $0 cost, so members actually know where they stand and can get the care they need without surprise bills or medical debt,” Mr. Turner said in the release.
According to the news release, Curative plan members will not owe any copay costs if they complete a baseline visit to evaluate preventive care and health literacy.
From the Postal Service front, Federal News Network reports
Postmaster General Louis DeJoy announced Wednesday that all Executive and Administrative Schedule (EAS) and Pay Band Non-bargaining unit employees will soon receive a 3% salary increase, “regardless of their current salary maximum.”
DeJoy, in a memo to USPS officers Wednesday, said the pay increase will go into effect Sept. 24 and will reflect on the employees’ Oct. 14 pay statement.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.