Tuesday’s Tidbits

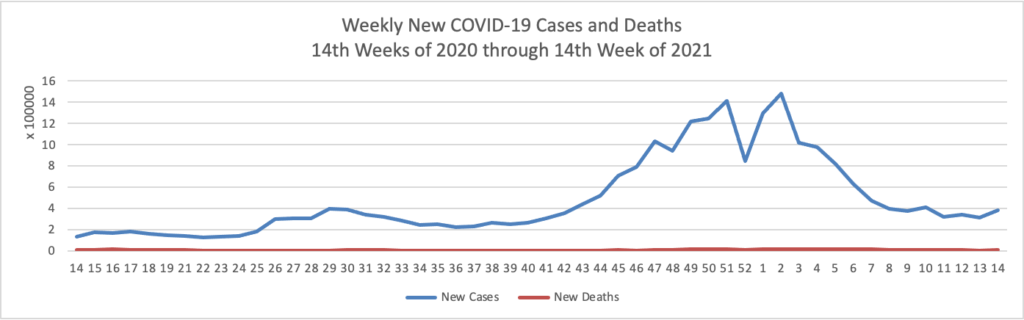
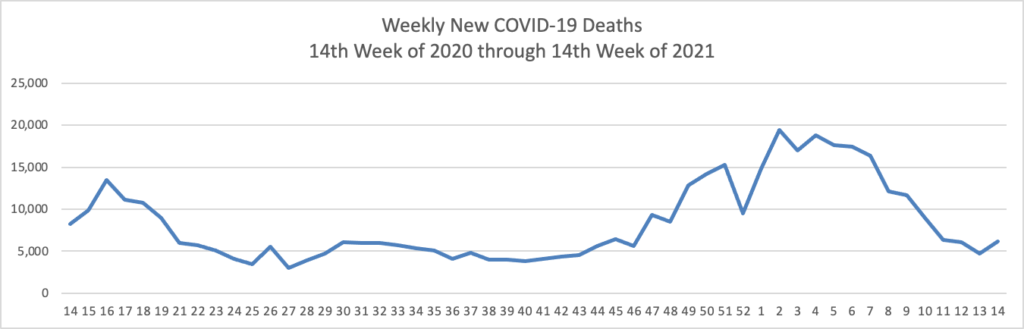
From the COVID-19 front
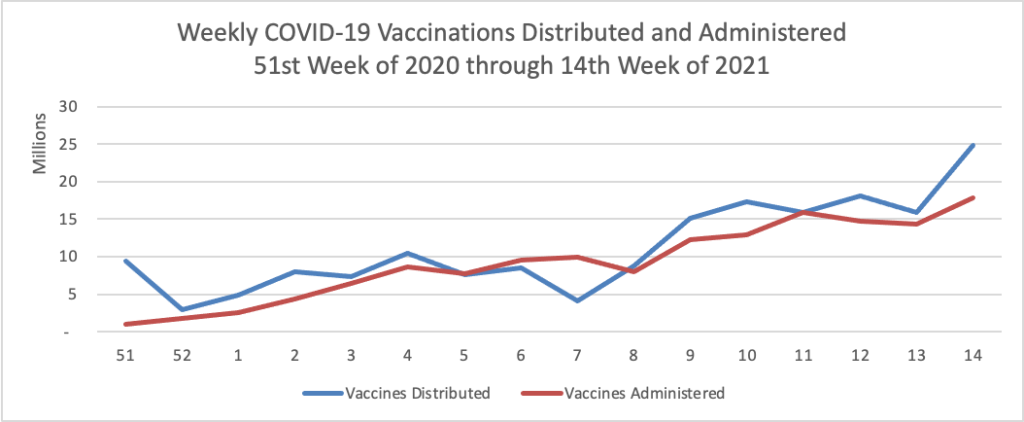
- The Hill informs us that “President Biden on Tuesday pleaded with Americans to get vaccinated against COVID-19 as the White House signaled a shift toward grassroots tactics to reach those who have yet to get a shot.” Here is a link to the President’s full remarks.
- NPR Shots offers a daily look at each state’s progress in vaccinating its residents.
From the hospital pricing transparency front —
- The Wall Street Journal explains how it has been analyzing the pricing data that federal law required hospitals to make publicly available on January 1, 2021. “The Journal reviewed hospital pricing disclosures collected by Turquoise Health Co., a startup that has been gathering the data from hospital websites since the regulations went into effect.” The Turquoise Health website is worth a gander.
- NPR Shots also analyzed the newly available hospital pricing data. “While it’s still an unanswered question about whether price transparency will lead to overall lower prices, KHN took a dive into the initial trove of data to see what it reveals. Here are five takeaways from the newly public data and tips for how you might be able to use it to your benefit: 1) As expected prices are all over the map; 2. Patients can look up information but the info is incomplete; 3. Third party firms like Turquoise Health are trying to make searching prices simpler and cash in; 4. Consumers can use the data to negotiate with hospitals when paying cash, and 5. Hospitals are not fully on board currently.
In the tidbits department —
- Today, the Centers for Medicare and Medicaid Services announced Dr. Meena Seshamani, M.D., Ph.D. [formerly with MedStar Health] as Deputy Administrator and Director of Center for Medicare. She started her work today.
- Fierce Healthcare reports “The United Health Foundation, the philanthropic arm of the UnitedHealth Group, released its America’s Health Rankings Health Disparities Report last week, and the healthcare giant found a number of disparities worsened in the 2017 to 2019 time frame. While the data come from before the pandemic, experts say they offer a baseline that can be used to address critical public health needs. For example, adults who did not graduate high school had a rate of frequent mental distress that was 123% higher than people with a college degree. Females had a 70% higher rate of depression than males, according to the report.”
- NPR Shots discusses how an “obesity drug’s [Wegovy] promise now hinges on insurance coverage.”
In clinical trials, weekly injections of semaglutide — or Wegovy, as it’s been branded — helped people drop an average of 15% of their body weight. That’s an average of about 34 pounds over 16 months, before their weight plateaued, a far greater weight loss, obesity specialists say, than achieved with other drugs on the market. At least as important, Wegovy raised none of the alarm bells with the FDA or obesity doctors that it might trigger serious side effects of the sort some people experienced by taking fen-phen or other previous medical treatments for obesity.
But with a price tag for Wegovy of $1,000 to $1,500 a month, a big question remains: Will insurers cover its significant cost for the millions who might benefit? * * *
Insurance coverage, it turns out, is a giant question — not just with Wegovy but with obesity drugs in general. Some private insurers do include some prescription obesity drugs in the list of medicines they’ll cover; it’s too early to tell whether Wegovy will make those lists. Many doctors and patients are optimistic, because it is a higher dose of an existing diabetes medication called Ozempic, which insurers often cover.
A few select state Medicaid programs will cover medications that treat obesity in some circumstances. But, significantly, Medicare does not cover obesity drugs — and many private insurers typically follow Medicare’s lead.
Yet the demand for a good treatment is there, says Dr. Fatima Cody Stanford, a leading obesity researcher at Harvard. She was not involved in conducting the Wegovy clinical trial but closely followed it. “I’m excited about it,” she says, because of the dramatic weight loss.
The drug acts on the brain so people eat less and store less of what they eat. That helps address the excess weight as well as helping with related diseases of the liver or heart, for example.
- The FEHBlog enjoys book recommendations and so he lapped up STAT’s list of “the 36 best books and podcasts on health and science to check out this summer. Among them, this one particularly caught the FEHBlog’s attention as he has enjoyed reading this author’s output and the topic is intriguing: “The Code Breaker: Jennifer Doudna, Gene Editing, and the Future of the Human Race” By Walter Issacson I recommend it because this captivating book provided clear and accessible explanations of the scientific discovery of CRISPR-Cas9 and its remarkable power as a gene editing tool, interwoven with the complex human stories of Jennifer Doudna and her relationships with the many other accomplished scientists who brought it all together.— Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases”