Monday Roundup

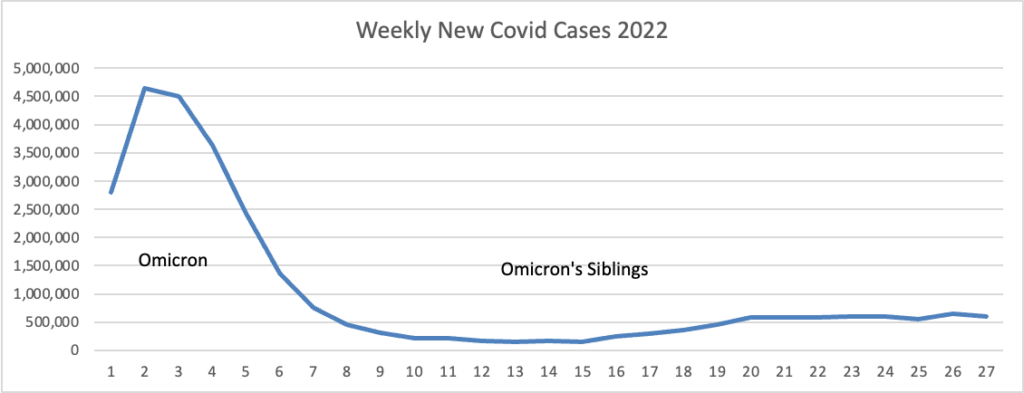
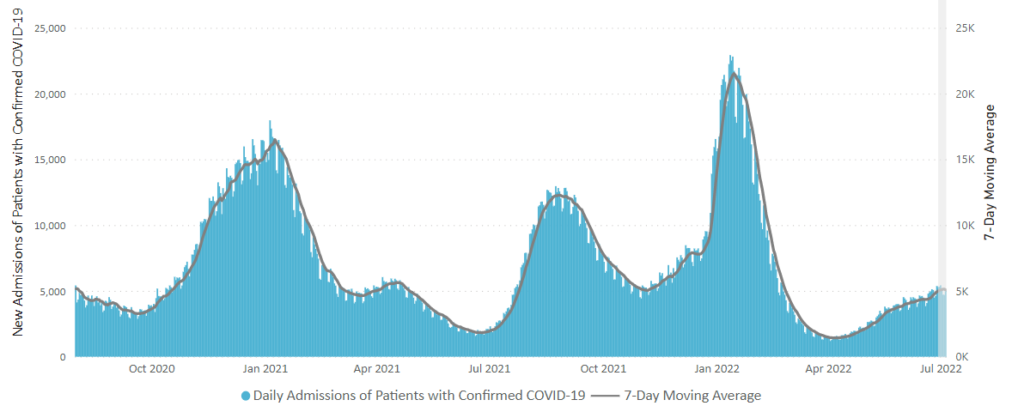
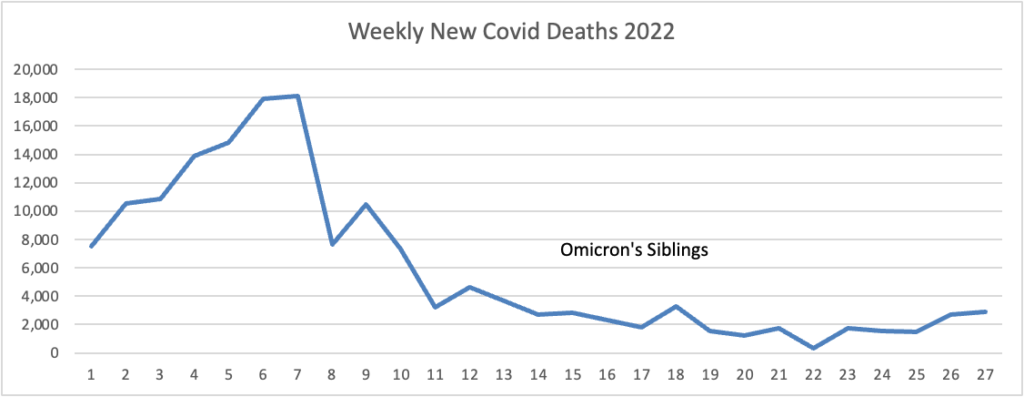
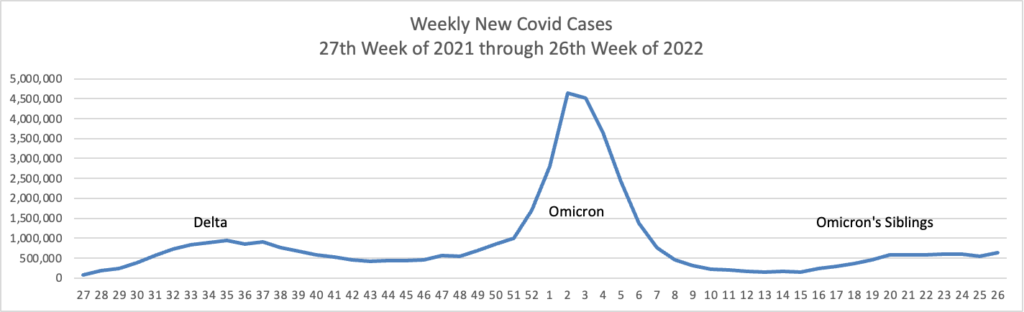
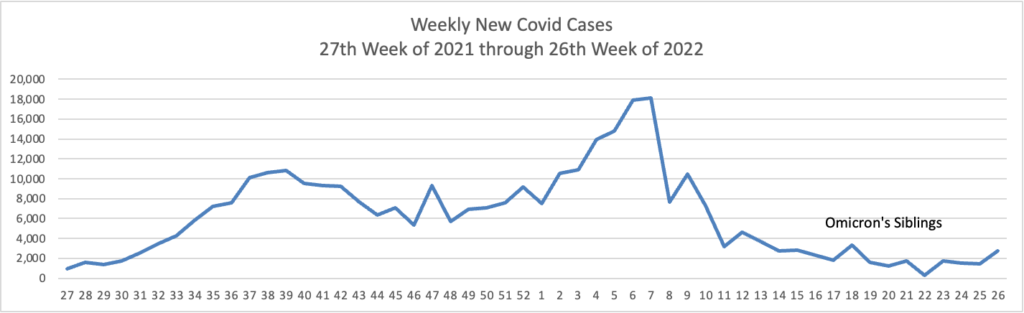
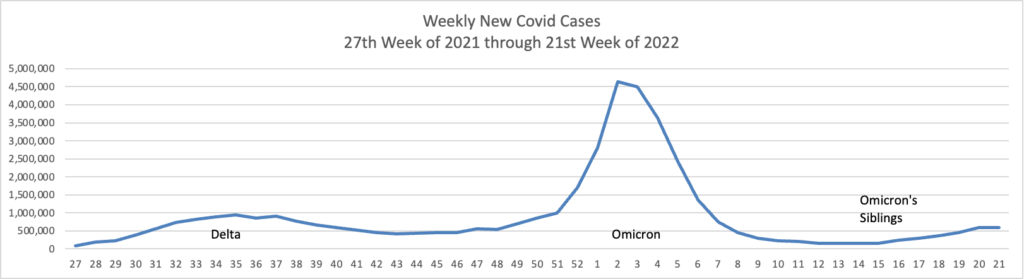
From the Omicron and siblings’ front
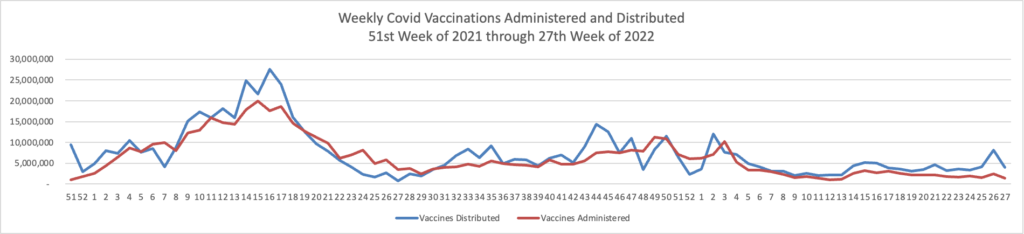
- The CDC’s Advisory Committee on Immunization Practices will take up the FDA’s grant of emergency use authorization to the Novovax traditionally developed Covid vaccine tomorrow.
- The American Hospital Association tells us “Two doses of the Pfizer or Moderna COVID-19 vaccine were less effective at preventing hospitalizations during the omicron BA.2 and BA.2.12.1 periods than during the BA.1 period, but a third and fourth dose provided additional protection to eligible adults, the Centers for Disease Control and Prevention reported Friday.”
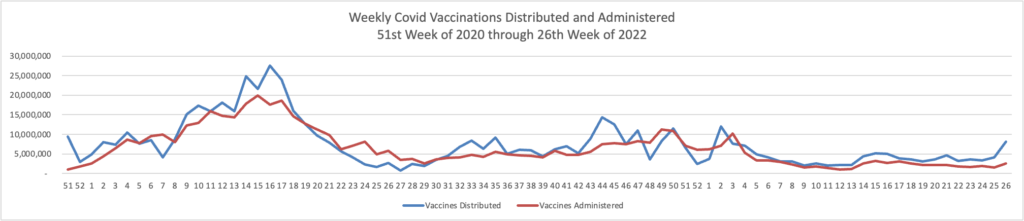
- “Getting vaccinated now will not prevent you from getting an authorized variant-specific vaccine in the fall or winter when they are recommended for you,” CDC said. “Given recent increases in deaths and hospitalizations associated with the BA.5 variant, everyone should stay up to date with recommended COVID-19 vaccinations, including additional booster doses for those who are moderately to severely immunocompromised and adults over 50.”
Also from the public health front, Medscape reports
Iron accumulation in the brain as a result of alcohol consumption may explain why even moderate drinking is linked to compromised cognitive function.
Results of a large observational study suggest brain iron accumulation is a “plausible pathway” through which alcohol negatively affects cognition, study Anya Topiwala, MD, PhD, senior clinical researcher, Nuffield Department of Population Health, University of Oxford, Oxford, England, told Medscape Medical News.
Study participants who drank 56 grams of alcohol a week had higher brain iron levels. The UK guideline for “low risk” alcohol consumption is less than 14 units weekly or 112 grams.
The study was published online June 14 in PLOS Medicine.
The National Institutes of Health announced
Research supported by the National Institutes of Health shows that cardiovascular-related deaths have declined over the past two decades, but disparities remain. Researchers found that inequities are mostly driven by differences in race and ethnicity, geographic location, and access to care, among other factors. The findings were published in Circulation, and the research was partially funded by the National Heart, Lung, and Blood Institute (NHLBI), part of NIH.
In one paper(link is external), researchers analyzed data from the Centers for Disease Control and Prevention and found that, after adjusting for age, rates of cardiovascular disease-linked deaths dropped among Black and white adults between 1999 and 2019, as did heart disease-related disparities between the two groups. However, Black adults continue to experience higher death rates than white adults, especially in rural or segregated areas, according to the researchers.
From the Medicare front, Healthcare Dive informs us
Federal health regulators want to increase hospital outpatient payments by 2.7% for 2023, an increase of about $6.2 billion in Medicare payments from this year.
Yet, the American Hospital Association is “deeply concerned” about the proposed Medicare payment rate amid increased inflation.
“A much higher update is warranted,” AHA Executive Vice President Stacey Hughes said in a Friday statement following the release of the proposed 2023 Hospital Outpatient Prospective Payment System rule.
Circular logic, like the AHA’s here, feeds inflation in the FEHBlog’s view.
From the U.S. healthcare business front, MedPage Today reports “A growing demand for specialty services is once again spurring a bump in starting salaries for specialty physicians, according to a new report from AMN Healthcare and its physician search division, Merritt Hawkins. ‘Demand for physicians, and the salaries they are offered, have rebounded dramatically from the height of COVID-19,’ AMN’s president of physician permanent placement, Tom Florence, said in a statement. ‘Virtually every hospital and large medical group in the country is looking to add physicians.'”
From the health insurance literacy front, Benefits Pro observes
Despite spending more than $1 trillion on health insurance each year, many U.S. consumers are making poorly informed decisions – and paying for their lack of understanding.
According to the latest Health Insurance Literacy Survey from HealthCare.com:
* 1 in 4 Americans say lack of health insurance understanding caused them to receive a higher-than-expected medical bill.
* Half believe that copays count toward deductibles when they generally do not.
* Half of the respondents say they can’t afford health insurance without employer coverage.
* 3 in 10 stay in jobs they don’t like or take jobs they don’t want so they can receive health insurance.
The survey of 1,000 consumers younger than 65 identified several broad areas of concern, including confusion and complexity and unfounded confidence.