The continuing resolution funding the federal government expires at 11:59 pm on Friday December 16.
The Federal Employee Benefits Open Season ends at 11:59 pm, in the location of the enrollee’s electronic enrollment system, on Monday, December 12, 2022.
The Medicare Open Enrollment period ends this Wednesday, December 7.
From the Rx coverage front, the Wall Street Journal reports on
A shortage in the weight loss drug Wegovy, “missing out on hundreds of millions of dollars in sales and squandering a head start before a rival could begin selling a competing product. * * * [Wegovy manufacturer’ Novo lists Wegovy at $1,349 a month. Some commercial insurers cover the drug.” OPM has encouraged FEHB carriers to offer coverage of this drug.
A CVS Health effort to improve pharmacy efficiency with “a system [currently being tested] that allows pharmacists to process prescriptions in part remotely, a move it said could improve store working conditions and the experience for customers as the company grapples with a shortage of pharmacists.”
From the mental healthcare front, Health Payer Intelligence tells us
Mental healthcare services utilization and network size have grown significantly since 2019 among Blue Cross Blue Shield of Massachusetts (“Blue Cross”) members, according to data from Blue Cross.
Mental healthcare services utilization grew by 100 percent in the timeframe that Blue Cross examined. At the same time, Blue Cross’s mental healthcare network grew by 46 percent.
“As the need for mental health services continues to grow, access to convenient and affordable care is critical,” said Andrew Dreyfus, president and chief executive officer of Blue Cross. “By expanding and diversifying our mental health network, we’re ensuring that our members are able to find and receive the high-quality care they need, when they need it.”
The mental healthcare provider network swelled to a total of 18,000 clinicians. With the growth in utilization, Blue Cross plans to expand its network further. The payer will do this by working with national mental healthcare provider groups as well as expanding its virtual care mental health groups in 2023. * * *
Also worth reading is this Journal article about a 24-year-old military wife who went through drug addiction hell and came out a new person with help from her family, the Missouri prison where she was housed, and a fellow inmate. The article illustrates the importance of Blue Cross of Massachusett’s efforts to expand mental health coverage and various efforts to reduce drug addiction and overdose deaths.
From the medical research front, the Wall Street Journal offers an essay about breast cancer written by a medical historian and breast cancer patient Dr. Lindsey Fitzharris. What grabbed the FEHBlog’s eye is the article’s conclusion:
The cofounders of BioNTech recently announced that vaccines targeting cancer may be available before the end of the decade. Researchers at Duke University are already developing a vaccine that targets mutations commonly arising in people with certain types of advanced breast cancer. Using the same mRNA technology deployed against Covid-19, these types of vaccines would not be administered prophylactically but, rather, used as a treatment to trigger a stronger immune response in patients with locally recurrent or metastatic disease. When it comes to conquering breast cancer, future medical historians will have plenty to write about.
From the innovation front, Senior Living explains how to use Apple AirPods as hearing aids. MedTech Dive adds
Apple AirPods Pro earbuds have the potential to be a hearing aid for adults with mild to moderate hearing loss, according to a paper published in iScience.
Researchers found the earbuds meet four of the five standards for personal sound amplification products and perform comparably to hearing aids in terms of speech perception in quiet environments.
The study suggests that some consumer earbuds can function as hearing aids to potentially further lower the cost and address the stigma associated with the technology.
It’s also worth calling attention to the HHS Agency for Healthcare Quality and Research’s Effective Health Care Program’s website.
The Effective Health Care (EHC) Program improves the quality of health care by providing the best available evidence on the outcomes, benefits and harms, and appropriateness of drugs, devices, and health care services and by helping health care professionals, patients, policymakers, and health care systems make informed health care decisions. The EHC Program achieves this goal by partnering with research centers, academic institutions, health professional societies, consumer organizations, and other stakeholders to conduct research, evidence synthesis, evidence translation, dissemination, and implementation of research findings.
From the Omicron and siblings front, the Centers for Disease Control’s weekly interpretative summary of its Covid statistics explains
Cases
As of November 30, 2022, the current 7-day average of weekly new cases (43,300) decreased 1.2% compared with the previous 7-day average (43,837). A total of 98,777,220 COVID-19 cases have been reported in the United States as of December 30, 2022.
Variant Proportions
CDC Nowcast projections* for the week ending December 3, 2022, estimate the proportion of lineages designated as Omicron with estimates above 1%: BA.5—and four of its sublineages (BQ.1, BQ.1.1, BF.7, and BA.5.2.6)—BA.4.6,and XBB. XBB is a recombinant of two BA.2 sublineages.
New Hospital Admissions
The current 7-day daily average for November 23–29, 2022, was 4,201. This is a 17.6% increase from the prior 7-day average (3,572) from November 16–22, 2022.
Vaccinations
As of November 30, 2022, 655.3 million vaccine doses have been administered in the United States. Overall, about 267.3 million people, or 80.5% of the total U.S. population, have received at least one dose of vaccine. About 228.4 million people, or 68.8% of the total U.S. population, have completed a primary series.
Of those who have completed a primary series, about 114.8 million people have received a booster dose,* and more than 39.7 million people have received an updated (bivalent) booster dose. But 48.3% of the total booster-eligible population has not yet received a booster dose. Learn more about who is eligible.
Deaths
The current 7-day average of new deaths (254) decreased 32.4% compared with the previous 7-day average (376). As of November 30, 2022, a total of 1,077,303 Covid-19 deaths have been reported in the United States
The CDC also released an encouraging report about Paxlovid’s efficacy.
Summary
What is already known about this topic?
Nirmatrelvir-ritonavir (Paxlovid) is an outpatient antiviral medication recommended for adults with mild-to-moderate COVID-19 who have elevated risk of severe illness.
What is added by this report?
Among U.S. adults diagnosed with COVID-19, including those with previous infection or vaccination, persons who were prescribed Paxlovid within 5 days of diagnosis had a 51% lower hospitalization rate within 30 days after diagnosis than those who were not prescribed Paxlovid.
What are the implications for public health practice?
Paxlovid should be offered to eligible adults irrespective of vaccination status, especially in groups with the highest risk for severe COVID-19 outcomes, such as older adults and those with multiple underlying health conditions.
Also from the public health front, the CDC’s Fluview tells us
Seasonal influenza activity is high and continues to increase across the country.
Of influenza A viruses detected and subtyped this season, 79% have been influenza A(H3N2) and 21% have been influenza A(H1N1).
Two influenza-associated pediatric deaths were reported this week, for a total of 14 pediatric flu deaths reported so far this season.
CDC estimates that, so far this season, there have been at least 8.7 million illnesses, 78,000 hospitalizations, and 4,500 deaths from flu.
The cumulative hospitalization rate in the FluSurv-NET system is higher than the rate observed in week 47 during every previous season since 2010-2011.
The number of flu hospital admissions reported in the HHS Protect system during week 47 almost doubled compared with week 46.
The majority of influenza viruses tested are in the same genetic subclade as and antigenically similar to the influenza viruses included in this season’s influenza vaccine.
All viruses collected and evaluated this season have been susceptible to influenza antivirals.
An annual flu vaccine is the best way to protect against flu. Vaccination helps prevent infection and can also prevent serious outcomes in people who get vaccinated but still get sick with flu.
CDC recommends that everyone ages 6 months and older get a flu vaccine annually. Now is a good time to get vaccinated if you haven’t already.
There are also prescription flu antiviral drugs that can be used to treat flu illness; those need to be started as early as possible.
The Wall Street Journal offers a helpful overview of the tripledemic situation.
Scientific meetings about Alzheimer’s disease can be funereal affairs, with researchers from around the world gathering in hopes that the latest in a long line of negative clinical trials might light the path to a long-awaited success.
This year was different. Nearly 2,000 people showed up to the Clinical Trials in Alzheimer’s Disease meeting, a conference record, to hear about lecanemab, a drug from Eisai and Biogen that appears to have broken the decades-long cycle of disappointment.
A packed audience repeatedly burst into applause during Eisai’s lecanemab presentation on Tuesday — with onlookers clapping even when they learned that the results had been concurrently published in the New England Journal of Medicine. Supplemental figures don’t usually don’t draw cheers, but the warm reception underscored how overjoyed researchers were to have any kind of success against Alzheimer’s, even a modest one. * * *
Several researchers compared this moment in Alzheimer’s research to the early days of cancer therapy or HIV treatment — the first drugs aren’t smash hits, but they’re something for scientists and doctors to build on and learn from.
“It’s not like you’ve won the war with lecanemab,” said Eric Siemers, chief medical officer of Acumen Pharma. “We’ve got a lot of work to do. But this is an inflection point. There’s no question about it.”
In that regard, BioPharma Dive points out lessons learned from testing a Roche drug similar to lecanermab.
After one year of treatment, [the Roche drug] gantenerumab reduced amyloid burden in patients only half as well as the trials’ designers had expected based on previous research, said researcher Randall Bateman, a neurology professor at Washington University in St. Louis who helped lead the studies.
Moreover, around half as many gantenerumab patients as predicted tested negative for amyloid over the course of the trial. Almost none tested negative after one year of treatment, and only around a quarter did after more than two years, researchers revealed.
Data for lecanemab and donanemab presented at CTAD, meanwhile, showed stronger amyloid clearance, helping boost confidence in those drugs.
Bateman also pointed to a post-study analysis researchers conducted of Roche’s trials that hinted at better outcomes for trial participants who had higher reductions in amyloid, although this finding wasn’t statistically conclusive.
Taken together with data from other trials, gantenerumab’s results should help researchers as they try to optimize available therapies and develop new ones, Bateman said.
“I see this as one of the missing essential pieces of the puzzle of figuring out how to optimally treat along this pathway for amyloid removal,” he said.
Meanwhile, the New York Times tells us about “A Promising Trial Targets a Genetic Risk for Alzheimer’s Preliminary results offer hope that gene therapy can protect people with a version of the brain disease driven by a particular gene variant.”
From the U.S. healthcare business front, Healthcare Dive reports
Advocate Aurora Health and Atrium Health announced Friday the two providers have closed their merger deal, becoming the nation’s fifth-largest nonprofit health system by revenue.
The new system, Advocate Health, will generate revenue of more than $27 billion and operate 67 hospitals and more than 1,000 sites of care in six states. The system expects to treat nearly 6 million patients each year. * * *
Instead, economists told Healthcare Dive, the FTC is likely to examine insurer overlap in the case of Advocate Health. The combined entity operates in Illinois, Wisconsin, Georgia, North Carolina, South Carolina and Alabama.
The Biden administration will allow agencies to hire employees in certain positions on a temporary basis for up to 10 years, more than doubling the current cap limiting the assignments for those workers.
The Office of Personnel Management issued the rule on Thursday, finalizing a proposal first put forward by the Trump administration. The rule will enable federal agencies to appoint employees in STEM jobs for a decade. OPM said the change would give agencies more flexibility when tackling long-term science, technology, engineering and mathematics projects. Previous regulations required agencies to get special permission from OPM to keep any term employee on staff for longer than four years.
Viet Tran, an OPM spokesman, said the rule showed the administration’s “commitment to STEM hiring.” He added it would allow for more federal, rather than outsourced, hiring.
“With this final rule, agencies have more flexibility and support (and less administrative burden) to hire employees—rather than contractors—for non-permanent STEM positions that agencies expect from the outset to last longer than 4 years but not more than 10 years,” Tran said. “This is another tool to help agencies better compete for talent.”
As the FEHBlog has explained, federal employees can expect a 4.6% pay raise for 2023 with 4.1% of the increase being distributed across the GS schedule and the remaining 0.5% allocated to locality pay. As it turns out, the Society for Human Resource Management tells us
Employers in the U.S. plan to boost salaries an average of 4.6 percent in 2023, up from 4.2 percent this year, according to a new study.
Employers say inflationary pressures and the ongoing challenges of finding and keeping workers are the main reasons for the higher projected increases. Indeed, 3 in 4 of the 1,550 U.S. employers in the latest Salary Budget Planning Report by consultancy WTW say they continue to experience problems attracting and retaining workers.The survey was conducted from Oct. 3 to Nov. 4, 2022.
From the plan design front, a recent Kaiser Family Foundation report explains the growing use of all sizes of employers to provide retiree health benefits through Medicare Advantage plans.
This analysis uses data from the 2022 KFF Employer Health Benefits Survey to examine the extent to which large private and non-federal public employers that offer retiree health benefits are turning to Medicare Advantage and why they are making this shift. However, the Survey does not include information about union-administered benefits. For additional information about methods, see Survey Design and Methods.
Based on the Survey, we find:
Half (50%) of large employers offering retiree health benefits to Medicare-age retirees offer coverage to at least some retirees through a contract with a Medicare Advantage plan, nearly double the share in 2017 (26%).
About 44% of large employers that offer Medicare Advantage coverage to their retirees do not give retirees a choice in coverage options.
Among larger employers with 1,000 or more workers that offer retiree health benefits through a Medicare Advantage plan, the most commonly cited reason they elected this option was the lower cost.
FEHB plans also are implementing integrated Medicare Advantage plans as a cost-saving measure.
From the HHS front, “Today, the U.S. Department of Health and Human Services (HHS) Secretary Xavier Becerra marked the one-year anniversary of HHS’s Overdose Prevention Strategy (Strategy) by announcing the progress the nation has made since the release of the Strategy, showing expanded treatment capacity, lives saved from an overdose, and commitment to long term recovery supports.” Kudos. Here is the fact sheet.
From the Federal Employees Benefit Open Season front, Tammy Flanagan, writing in Govexec, explains the relationship between FEHB and Medicare coverage for the benefit of annuitants over age 65.
From the OPM front, Govexec and Federal News Network discuss an OPM management report released yesterday that includes more details on OPM’s 2022 Federal Employee Viewpoint Survey.
From Capitol Hill, Medpage Today informs us that “Telehealth, Mental Health Likely Topics for the New Congress in 2023, Experts Say.” In this regard, today the bipartisan leadership of the Senate Finance Committee “released a [fifth and final mental health parity] discussion draft including policies aimed at improving mental health parity in Medicare and Medicaid and helping to put access to mental health and substance use disorder (SUD) services on par with physical health care. Mental health parity includes a set of laws aimed at ensuring mental and physical health care are covered equally by health insurance. * * * The full text of the discussion draft is available here. A summary of all provisions released by the committee as a part of the bipartisan mental health effort, including mental health parity, is available here.”
COVID-19 hospitalizations have ticked up nationwide in recent weeks amid concerns of a potential winter surge, according to data tracked by The New York Times.
As of Nov. 29, the nation’s daily hospitalization average was 31,125, up 12 percent over the last 14 days. This figure is still down significantly from the more than 800,000 daily hospitalizations recorded during the peak of last winter’s omicron surge.
People with acute respiratory illness during the pandemic suffered similar levels of poor well-being in the months afterward whether they tested positive for SARS-CoV-2 or not, a registry study showed.
In a cohort of people who all had initial symptoms suggestive of COVID-19, those who had moderate to severe scores at 3 months on the pain, mood, and other quality-of-life measures on the Patient-Reported Outcomes Measurement Information System (PROMIS) scale were actually less likely to have tested positive for the coronavirus as to have had other causes of illness (39.6% vs 53.5%, P<0.001).
From the public health front —
MedPage Today explains how patients can try to distinguish among different respiratory illnesses, including RSV and the flu because at home testing is unavailable.
The Biden administration looks to end its public health emergency declaration for mpox — the virus formerly known as monkeypox until recently — a sign that officials believe they’ve brought the unprecedented outbreak under control, POLITICO’s Adam Cancryn reports.
Health officials are likely to issue a 60-day notice later this week for winding down the declaration, two people with knowledge of the matter told POLITICO, putting it on track to expire by Jan. 31. The decision isn’t yet final and could still change, the people cautioned. * * *
Some administration officials see the potential unwinding of the mpox emergency declaration as a test run for eventually ending the yearslong Covid emergency — a more complex challenge — that Biden aides expect to happen at some point next year.
From the Affordable Care Act and No Surprises Act front
The American Hospital Association (“AHA”) informs us
The Centers for Medicare & Medicaid Services seeks public input on topics related to essential health benefits — items and services that all non-grandfathered health plans in the individual and small group markets must cover under the Affordable Care Act. The agency is requesting feedback on how essential health benefits may need to be updated to reflect changes in medical evidence and scientific advancement, address gaps in coverage and health equity, or remove barriers to accessing services. In particular, CMS seeks feedback on essential health benefits related to maternal health, behavioral health and prescription drug coverage. The agency will publish the request for information in the Dec. 2 Federal Register, with comments accepted for 60 days.
and
AHA today urged the Centers for Medicare & Medicaid Services not to establish a national directory of health care providers and services (NDH) at this time.
“The AHA shares CMS’ goals to improve patient access to provider information and to facilitate health information exchange and data reporting,” the association wrote. “We appreciate the commitment CMS has invested in striving to meet these objectives. However, we are concerned that adding one more provider directory requirement will not support patients in accessing the information they need about their care providers. In fact, adding an additional data source without sufficiently addressing how or why it differs from the myriad provider directories already in existence could further complicate patients’ ability to access accurate information. Meanwhile, such a requirement would add considerable, duplicative burden on providers. Additionally, we have significant reservations about the current state of readiness of the essential technology needed for a centralized data hub such as the NDH.”
Mercer Consulting offers insights on the prescription drug and healthcare spending reports that health plans must submit to the federal government by December 27. Jingle bells.
Healthcare Dive reports that the Texas Medical Association has filed another lawsuit challenging different aspect of the independent dispute resolution rule. Haven’t the TMA lawyers heard about the opportunity available under the Federal Rules of Civil Procedure to amend their existing complaint?
The Food and Drug Administration approved the first therapy using bacteria from stool samples to treat a bowel disorder on Wednesday, paving the way for several similar treatments in development.
The drug, called Rebyota, is given as a one-dose treatment for Clostridium difficile infections, commonly known as C. diff., in which the toxin-producing bacteria disrupts the normal balance in a person’s digestive system. Rebyota is designed to restore balance by introducing good bacteria taken from donor stool samples.
“We are delighted that FDA has approved the first fecal microbiome restoration therapy for recurrent C. diff. This is an enormous step forward for the nearly 200,000 people who battle rCDI each year,” said Christian John Lillis, the executive director of the C. diff advocacy organization the Peggy Lillis Foundation.
Amgen released detailed data on Thursday suggesting an early-stage drug can induce significant weight loss in patients with obesity, with less frequent dosing than current treatments but a safety profile that remains unclear.
The results for the molecule, codenamed AMG133, throw Amgen in a long-gestating race with other major drugmakers that burst into the popular press this year.
Eli Lilly and the diabetes giant Novo Nordisk both market drugs that were recentlyshown to lower body weight by around 15% to 20% after a little over a year. (Lilly’s is currently approved only for diabetes, but it plans to submit for obesity next year.) The injectables have been highly sought after by both obesity specialist physicians, who have long searched in vain for something safe and effective to offer their patients, and celebrities hoping to look svelte in their next appearance.
From the miscellany department —
Beckers Hospital Review interviews a Kaiser Permanente expert about their successful use of remotely monitoring patients with diabetes and high blood pressure. The monitors deliver their results to Kaiser Permanente’s electronic health records for 40,000 members. Kudos.
Beckers also lets us know about large hospital systems that are having a profitable 2022.
Elon Musk’s brain-machine interface company Neuralink aims to put its first implant in a human subject in the next six months, he said during an event Wednesday.
Musk said the company has been “working hard to be ready for our first human,” and has submitted most of the required paperwork to the Food and Drug Administration to launch a study in humans. The company — which is designing a device to translate the brain’s signals into actions — also announced it will first focus specifically on two applications: restoring human vision, and helping people who can’t move their muscles to control devices like smartphones or even return the ability to move to people with severed spinal cords, Musk said.
Though it’s starting with certain parts of the brain, Musk said Neuralink’s long-term goal is to create a system that can translate impulses from the entire brain into actions.
The HCP-LAN, which promotes alternate / value-based payment methods, held a summit this week. RevCycle Intelligence reports
Photo by Josh Mills on Unsplash
Value-based payment levels barely moved in 2021, with some movement in the downside financial risk category, according to the latest data from the Health Care Payment Learning and Action Network (HCP LAN).
The majority of healthcare payments—59.5 percent—from 63 commercial plans, five state Medicaid programs, and Medicare were tied to value and quality in some capacity, the annual APM Measurement Effort report showed this year. The remaining 40.5 percent of payments stemmed from fee-for-service models.
The proportion of healthcare payments in fee-for-service models is actually up slightly from the 2020 results when 39.3 percent of payments were tied to the models. However, this does not indicate a backslide for the healthcare industry, according to value-based care expert Andréa E. Caballero, MPA.
Healthcare Dive looks forward to the HLTH conference that will be held in Las Vegas next week. “Representatives from major healthcare players will discuss private equity, value-based care, digital health funding and more at the fifth annual conference.”
From the Federal Employees Benefits Open Season front, FedWeek discusses the interaction of FEHB and Medicare.
Infants under 6 months old had the highest COVID-19 hospitalization rates among Americans under age 65 during March 20-Aug. 31, when the omicron BA.2 and BA.5 variants predominated, the Centers for Disease Control and Prevention reported today. Based on data from the COVID-19-Associated Hospitalization Surveillance Network, the study found infants under 6 months old had hospitalization rates similar to adults aged 65-74.
“COVID-19 vaccination during pregnancy might provide protection to infants younger than 6 months old who are currently ineligible for vaccination,” CDC said. “To protect themselves and their infants, people who are pregnant, breastfeeding, trying to get pregnant now, or might become pregnant in the future should stay up to date on COVID-19 vaccinations, as recommended by CDC and the American College of Obstetricians and Gynecologists.”
High rates of hospitalization with RSV are hitting the youngest children especially hard, part of an unseasonably early surge in respiratory infections.
Some 3.0 people for every 100,000 were hospitalized with respiratory syncytial virus the week ended Nov. 5, according to federal data from 12 states. The rate is the highest since the winter just before the pandemic, when some 2.7 people per 100,000 were hospitalized in January 2020. The hospitalization rate declined from 3.4 hospitalizations per 100,000 in the week ended Oct. 29.
Babies under six months old have the highest RSV-related hospitalization rate, data from the Centers for Disease Control and Prevention show, at 145 hospitalizations per 100,000 infants. Infants six to 12 months old were hospitalized at a rate of 63 for every 100,000 children that age. For adults, the hospitalization rate is 0.6 per 100,000 people.
RSV is a common virus that most children encounter by their second birthday. Reinfections can occur at any age. Most people experience mild, cold-like symptoms and recover in a week or two. But RSV can be serious for some infants and older adults, causing bronchitis and pneumonia.
AstraZeneca PLC said it had dropped plans to submit its Covid-19 vaccine to the Food and Drug Administration for approval, ending a long-running ambition to eventually sell the shot in the U.S. despite initial setbacks.
The Cambridge, England-based pharmaceutical company said Thursday that there would likely be a lack of demand in the U.S., where it said primary vaccination needs had been met. It would continue to focus its efforts on ensuring the availability of the vaccine, called Vaxzevria, elsewhere, including seeking its approval as a booster shot, the company said.
The risk for death from infective endocarditis (IE) increased twofold among young U.S. residents aged 15 to 44 years during 1999 to 2020, according to a research letter published online Nov. 9 in the Journal of Internal Medicine.
Laura McLaughlin, M.D., from the Columbia University Irving Medical Center in New York City, and colleagues characterized trends in mortality rates from IE among young U.S. residents (aged 15 to 44 years) and in relation to drug abuse using the Multiple Cause of Death Data from the U.S. Centers for Disease Control and Prevention between 1999 and 2000. Age-adjusted mortality rates standardized to 2000 U.S. census per 100,000 persons were reported. * * *
“The number of young people in the United States who die of infective endocarditis is increasing, and the ongoing opioid epidemic, specifically injectable drug abuse, appears to be a significant cause,” a coauthor said in a statement.
The Centers for Disease Control released its current / 2021 National and State Healthcare-Associated Infections (HAI) Progress Report.
From the plan design front, the International Foundation of Employee Benefit Plans offers suggestions from an expert panel on four steps for evaluating your plan’s diabetes coverage.
From the mental healthcare front, the Senate Finance Committee released its “Fourth Bipartisan Discussion Draft on Mental Health Proposes More Integration Between Mental and Physical Health Care, Bolsters Crisis Care.” The bill appears to focus on Medicare and Medicaid coverage. The Committee explains
This discussion draft on the mental health integration is the fourth legislative draft the Finance Committee has released since kicking off its bipartisan mental health initiative. The first, released in May, focused on telehealth policies. The second, released in June, focused on youth mental health. The third, released in September, focused on expanding the mental health care workforce. Other discussion drafts may be released. The committee is committed to fully paying for any mental health package with bipartisan, consensus-driven offsets.
Mindfulness meditation worked as well as a standard drug for treating anxiety in the first head-to-head comparison.
The study tested a widely used mindfulness program that includes 2 1/2 hours of classes weekly and 45 minutes of daily practice at home. Participants were randomly assigned to the program or daily use of a generic drug sold under the brand name Lexapro for depression and anxiety.
After two months, anxiety as measured on a severity scale declined by about 30% in both groups and continued to decrease during the following four months.
Study results, published Wednesday in the journal JAMA Psychiatry, are timely. In September, an influential U.S. health task force recommended routine anxiety screening for adults, and numerous reports suggest global anxiety rates have increased recently, related to worries over the pandemic, political and racial unrest, climate change and financial uncertainties.
November is awareness month for diabetes and C. Diff. Looking back at October, Medscape informs us
Maintaining a healthy body weight, being physically active, and following a healthy dietary pattern can help women live longer after breast cancer diagnosis, according to a major new analysis of the latest research.
From the Federal Employee Benefits Open Season front, the Federal Times offers its consumer guide.
The Centers for Medicare & Medicaid Services [CMS] late today posted a final rule on its website that will increase Medicare hospital outpatient prospective payment system rates by a net 3.8% in calendar year 2023 compared to 2022. This update is based on a market basket percentage increase of 4.1%, reduced by 0.3 percentage points for productivity. [AHA calls the increase insufficient.] * * *
CMS finalized the payment policy for CY 2023 of average sales price (ASP) +6% for drugs and biologicals acquired through the 340B Program as a result of the unanimous Supreme Court decision in American Hospital Association v. Becerra.
CMS also finalized proposals to establish the Rural Emergency Hospital (REH) model, a new provider type for eligible critical access hospitals and small rural hospitals beginning in Jan. 1, 2023. The rule finalized proposals related to model payment, covered services, conditions of participation, and quality measurements.
[and]
The Centers for Medicare & Medicaid Services today released on its website its calendar year 2023 final rule for the physician fee schedule. The rule will cut the conversion factor to $33.06 in CY 2023 from $34.61 in CY 2022, which reflects the expiration of the temporary 3% statutory payment increase; a 0.00% conversion factor update; and a budget-neutrality adjustment.
CMS evaluated two and a half years of readmission cases for Medicare patients through the Hospital Readmissions Reduction Program and penalized 2,273 hospitals that had a greater-than-expected rate of return, according to a Nov. 1 report from Kaiser Health News.
The average payment reduction was 0.43 percent, the lowest rate reduction since 2014. Reductions will be applied to each Medicare payment to the affected hospitals from Oct. 1 through next September. It is expected to cost the hospitals $320 million over the 12-month period.
The report notes that the COVID-19 pandemic caused turmoil in hospitals and that CMS decided to exclude the first half of 2020 from the report due to the chaos. CMS also excluded Medicare patients who were readmitted with pneumonia across all three years because of the difficulty distinguishing them from COVID patients.
From the Affordable Care Act preventive services front, Healio tells us
The U.S. Preventive Services Task Force has released two final recommendations on the use of hormone therapy for the primary prevention of chronic conditions in postmenopausal people.
The recommendations advocate against the use of menopausal hormone therapy (MHT) through a combination of estrogen and progestin in postmenopausal people, and MHT through estrogen alone in postmenopausal people who have had a hysterectomy.
Both are D-grade recommendations and are consistent with the USPSTF’s previous recommendations on the treatment made back in 2017.
James Stevermer, MD, MSPH, a task force member, also noted in the press release that the recommendations are only for those who are considering hormone therapy to prevent chronic conditions following menopause.
“Those who wish to manage symptoms of menopause with hormone therapy are encouraged to talk with their health care professional,” he said.
From the prescription drug and vaccine development front —
Pfizer’s maternal vaccine against the respiratory syncytial virus [RSV] reduced the rate of severe illness in newborns by 81.8%, the company said Tuesday, meeting the goal of a pivotal study.
The company said that it plans to file the data on the vaccine with regulators by the end of the year and that it expects an eight-month review.
RSV is a common cause of illness and infection in young infants. By giving the vaccine during pregnancy, researchers hope antibodies generated by mothers would be transferred to infants. Currently, the pertussis vaccine and the influenza vaccine are given during pregnancy for this reason.
Vertex Pharmaceuticals, a Boston-based biotech company, * * * is testing a non-opioid drug for acute pain. Vertex’s drug, VX-548, aims to block the Nav1.8 sodium channel, which acts like a gate allowing pain signals to travel from the nerves to the brain.
VX-548 met its goals in late-stage trials evaluating the drug in people who underwent a bunionectomy or an abdominoplasty, the formal name for a tummy tuck. Vertex will run the same studies with more patients before seeking regulatory approval. The company hasn’t disclosed when data will be available beyond saying the trials will be quick since patients receive the drug for only 48 hours. Vertex is also testing VX-548 in nerve pain and eventually wants to see if it works for chronic pain.
If VX-548 passes its next big tests, it could offer a new option for people recovering from surgery or other medical procedures. Of course, plenty of other pain drugs that looked promising early on in testing never reached the market.
Fortunately, scientists are investing time and money on a variety of alternatives for pain.
From the Rx coverage front, BioPharma Dive relates
Eli Lilly’s new diabetes medicine Mounjaro outpaced Wall Street sales forecasts during the third quarter, fueled by strong patient demand and widening insurer coverage.
U.S. sales of the drug totaled $97 million between July and September, Mounjaro’s first full quarter on the market since its May 13 approval by the Food and Drug Administration. Payments related to a collaboration agreement with Mitsubishi Tanabe Pharma in Japan pushed global revenue for the quarter to $187 million, well above the consensus analyst forecast of $82 million.
“We have seen unprecedented demand for Mounjaro’s Type 2 diabetes launch in the U.S.,” said Anat Ashkenazi, Lilly’s chief financial officer, on a Tuesday call with analysts.
Lilly is also conducting a study to support an FDA marketing application for Mounjaro to be prescribed for weight loss.
Notably, Mounjaro showed a potent effect in reducing trial participants’ weight, a benefit that was also observed in a large study specifically assessing it as an obesity treatment. While it’s currently only approved to treat Type 2 diabetes, its potential as a medicine for both chronic conditions has made it one of Lilly’s most important products.
Lilly is currently conducting a second study in obesity and plans to complete an approval application in that indication should results, expected in April next year, also prove positive.
In U.S. healthcare business news, MedTech Dive reports
Johnson & Johnson agreed to acquire Abiomed, a Danvers, Mass.-based maker of heart pumps, for $16.6 billion.
The deal will contribute to J&J’s cardiovascular portfolio, complementing its Biosense Webster electrophysiology business, BTIG Analyst Marie Thibault wrote in a research note on Tuesday.
The deal has already been approved by both companies’ boards of directors and is expected to close before the end of the first quarter of 2023.
Finally, check out the NIH Director’s blog discussing “How the Brain Differentiates the ‘Click,’ ‘Crack,’ or ‘Thud’ of Everyday Tasks.”
If you’ve been staying up late to watch the World Series, you probably spent those nine innings hoping for superstars Bryce Harper or José Altuve to square up a fastball and send it sailing out of the yard. Long-time baseball fans like me can distinguish immediately the loud crack of a home-run swing from the dull thud of a weak grounder.
Our brains have such a fascinating ability to discern “right” sounds from “wrong” ones in just an instant. This applies not only in baseball, but in the things that we do throughout the day, whether it’s hitting the right note on a musical instrument or pushing the car door just enough to click it shut without slamming.
Now, an NIH-funded team of neuroscientists has discovered what happens in the brain when one hears an expected or “right” sound versus a “wrong” one after completing a task. It turns out that the mammalian brain is remarkably good at predicting both when a sound should happen and what it ideally ought to sound like. Any notable mismatch between that expectation and the feedback, and the hearing center of the brain reacts.
As the late Kenny Rogers sang, “You need to know when to hold them and when to fold them.” The FEHBlog tried to revive his Covid charts, but alas, it was infeasible because the FEHBlog could not show the stats in seven-day weeks as FEHBlog had been doing.
In any event, the Centers for Disease Control continues to issue weekly interpretations of Covid statistics so here we go:
New Reported Cases
As of October 26, 2022, the current 21-day average of weekly new cases (37,683) decreased 25.1% compared with the previous 21-day average (50,328). A total of 97,329,787 COVID-19 cases have been reported in the United States as of October 26, 2022.
CDC Nowcast projections* for the week ending October 29, 2022, estimate that the combined national proportion of lineages designated as Omicron will continue to be 100%. There are eight lineages designated as Omicron with estimates above 1%: BA.5—and four of its sublineages (BQ.1, BQ.1.1, BF.7, and BA.5.2.6)—BA.4.6, BA.2.75, and BA.2.75.2. The predominant Omicron lineage is BA.5, projected to be 49.6% (95% PI 45.3-53.9%).
The New York Times report on a study finding that Covid rebounds can happen to people have not taken Paxlovid.
“Symptom return is common,” said Dr. Davey Smith, the chief of infectious diseases and global public health at the University of California, San Diego School of Medicine, who led the study. “It doesn’t mean that things are going south. It’s just the natural way the disease goes.” What is surprising, however, is how many people may experience a rebound, he said. * * *
“The good news is that nobody who had their symptoms return needed to go to the hospital or died or even got severe symptoms,” Dr. Smith said. Eighty-five percent of those who had a rebound reported that their symptoms were mild; 15 percent had at least one moderate symptom. * * *
Concerns about rebound symptoms when taking Paxlovid — and another antiviral drug called molnupiravir — appear to have reduced people’s interest in using treatments for Covid. But the new study shows that you can have a rebound with untreated Covid as well. “I hope this can help people to be less afraid of a potential rebound,” Dr. Smith said.
If you do experience a rebound after treatment, there is no evidence that you need to start another course of Paxlovid. Isolate a while longer in case you are contagious to others. And try to manage symptoms with pain and fever-reducing medicines, home remedies and time, Dr. Smith said. “I recommend staying hydrated, watching ‘The Golden Girls’ and eating chicken soup.”
New Covid Hospitalizations
The current 7-day daily average for October 19–25, 2022, was 3,249. This is a 1.0% increase from the prior 7-day average (3,217) from October 12–18, 2022.
New Reported Deaths
The current 21-day average of new deaths (373) decreased 13.7% compared with the previous 21-day average (432). As of October 26, 2022, a total of 1,066,351 COVID-19 deaths have been reported in the United States.
Covid Vaccinations
As of October 26, 2022, 636.9 million vaccine doses have been administered in the United States. Overall, about 266.0 million people, or 80.1% of the total U.S. population, have received at least one dose of vaccine. About 226.9 million people, or 68.4% of the total U.S. population, have completed a primary series.
Of those who have completed a primary series, about 111.8 million people have received a booster dose,* and more than 22.88 million people have received an updated (bivalent) booster dose. But 49.3% of the total booster-eligible population has not yet received a booster dose. Booster dose eligibility varies by age and health condition.
CDC Community Levels
As of October 27, 2022, there are 73 (2.3%) counties, districts, or territories with a high COVID-19 Community Level, 705 (21.9%) counties with a medium Community Level, and 2,439 (75.8%) counties with a low Community Level. Compared with last week, this represents a minor increase (+0.8 percentage points) in the number of high-level counties, a minor increase (+4.4 percentage points) in the number of medium-level counties, and a minor decrease (-5.2 percentage points) in the number of low-level counties. Overall, 46 out of 52 jurisdictions** had high- or medium-level counties this week. California, Delaware, the District of Columbia, Hawaii, North Carolina, and South Carolina are the only jurisdictions to have all counties at low Community Levels.
Influenza activity continues to increase. Regions 4 (southeast) and 6 (south-central) are reporting the highest levels of flu activity.
The first influenza-associated pediatric death of the 2022-2023 season was reported this week.
CDC estimates that, so far this season, there have been at least 880,000 flu illnesses, 6,900 hospitalizations, and 360 deaths from flu.
The cumulative hospitalization rate in the FluSurv-NET system is higher than the rate observed in week 42 during previous seasons going back to 2010-2011.
An annual flu vaccine is the best way to protect against flu. Vaccination helps prevent infection and can also prevent serious outcomes in people who get vaccinated but still get sick with flu.
CDC recommends that everyone ages 6 months and older get a flu vaccine annually.
There are also prescription flu antiviral drugs that can be used to treat flu illness; those need to be started as early as possible.
An estimated 21% of adults have gotten a flu vaccine this year, similar to estimates from the same time last year, the CDC said, basing its estimates off an Ipsos survey conducted in early October. An estimated 22% of children have also gotten a flu shot, according to the CDC’s national immunization survey.
It is too early to tell how effective this year’s vaccine will be, the CDC said. But the influenza virus that is being most often reported, a strain of influenza A called H3N2, matches well with the formation of this year’s shot, health experts said.
The CDC has an updated RSV page with prevention and symptom guidance. Yahoo News adds “U.S. officials are working on a respiratory syncytial virus (RSV) vaccine, but until one is available people should exercise caution, especially seniors and parents of young children, the nation’s top infectious disease official said.”
In other virus news, Prescision Vaccinations discusses the severe impact that monkeypox infections can have on immunocompromised people, such as those with HIV or AIDs.
Following up on yesterday’s note on the Kaiser Family Foundation’s 2022 Employer Health Benefit Survey
Beckers Payer Issues calls four figures to our attention.
Kaiser Family Foundation delves into the survey’s findings about employer sponsored mental health programs.
From the U.S. healthcare business front, BioPharma Dive reports on Gilead’s third quarter earnings report.
The results [which exceeded Wall Street expectations] were, in part, tied to growing sales from Gilead’s cell therapy business, which consists of the marketed cancer drugs Yescarta and Tecartus. Together, sales from the two drugs totaled $398 million in the third quarter, a nearly 80% increase from the same three-month period a year prior. * * *
Third quarter sales of Tecartus were up 72% year over year, reaching $81 million, while those for Yescarta rose 81% to $317 million. Gilead cited the approval of Yescarta as a “second-line” therapy for a type of hard-to-treat lymphoma, which happened in April, as a main reason for the uptick.
Other cell therapy developers have recorded larger sales from their products as well, though not to the same extent as Gilead.
From the Medicare front, the Centers for Medicare and Medicaid Services announced issuing a
final rule that updates Medicare enrollment and eligibility rules to expand coverage for people with Medicare and advance health equity. The final rule, which implements changes made by the Consolidated Appropriations Act, 2021 (CAA), makes it easier for people to enroll in Medicare and eliminates delays in coverage. Among these changes, individuals will now have Medicare coverage the month immediately after their enrollment, thereby reducing any delays in coverage. In addition, the rule expands access through Medicare special enrollment periods (SEPs) and allows certain eligible beneficiaries to receive Medicare Part B coverage without a late enrollment penalty.
The Department of Health and Human Services will launch a national advertising campaign and tour to encourage families to get the updated Pfizer or Moderna COVID-19 vaccine booster to protect themselves against the omicron variants before winter and the holiday season, the White House announced today. As part of the tour, HHS will host pop-up vaccination events, and encourage others to share information on COVID-19 vaccines and host vaccination events.
Whereas alpha, beta, gamma and the other named variants sprouted new branches on the SARS-CoV-2 family tree, those limbs were dwarfed by the omicron bough, which is now studded with a plethora of subvariant stems.
“The children of omicron — so the many direct children and cousins within the diverse omicron family — those have displaced each other” as the dominant strains driving the pandemic, says Emma Hodcroft, a molecular epidemiologist at the University of Bern. “But that same family has been dominating” by outcompeting other strains.
The article delves into the future as well.
From the Rx coverage front —
Fierce Healthcare tells us that health insurer Centene announced its third-quarter results and a new PBM contract with Express Scripts.
Florida Blue Cross announced a mail-order pharmacy agreement with Amazon.
From the telehealth front —
The Federal Times discusses FEHB telehealth coverage available in 2023.
As federal employees prepare to make their selections for next year’s health insurance benefits, some may wonder whether telehealth services, made especially popular and necessary by the COVID-19 pandemic, will stick around.
For the most part, beneficiaries under the Federal Employee Health Benefits program will not see a major drop-off of telehealth options for 2023, said the White House’s Office of Personnel Management’s Edward DeHarde, who leads federal employee insurance operations, in an interview.
While the Federal Times article is focused on the hub and spoke telehealth services, STAT News considers the growing practice of pharmaceutical manufacturers making their drugs available to consumers through a third-party telehealth service.
From the tidbits department
The Wall Street Journal discusses the impact of health insurance spending on the consumer price index. In short, “The subindex of the consumer-price index is about to turn from a driver of inflation into a deflationary drag.”
The U.S. Public Health Service Task Force released for public comment a draft I (or inconclusive_ recommendation: “The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of visual skin examination by a clinician to screen for skin cancer in [asymptomatic] adolescents and adults.” The comment deadline is November 21, 2022.
CNN reports “One in 10 Americans over 65 had dementia, while 22% experienced mild cognitive impairment, the earliest stage of the slow slide into senility, according to a new study conducted between 2016 and 2017.” The study — the first in 20 years — breaks down its results by demographic categories.
My Federal Retirement offers its take on Medicare income adjusted premiums, known as IRMAA.
Employees and retirees are to be reminded that the IRMAA determination is usually based on Medicare Part B beneficiary’s federal income tax returns from two years earlier [e.g. 2021 governs 2023]. If a beneficiary’s income has dropped in the following year, then the beneficiary can appeal the IRMAA decision using Social Security Form SSA-44 (Medicare Income-Related Monthly Adjustment Amount -Life-Changing Event), providing proof that the beneficiary has experienced a “life-changing” event such as the death of a spouse or a divorce resulting in a significant decrease in income in the following year.
This is Red Ribbon Week, “an ideal way for people and communities to unite and take a visible stand against drugs.”
Speaking of illegal drugs, the Wall Street Journal tells the stories of three “high achieving” New York City dwellers who died on one day in March 2021 due to fentanyl-laced cocaine delivered by a single dealer.
New York City authorities have been warning of the risks of unknowingly taking fentanyl in cocaine and of its increased presence in cocaine seized by police. Health officials put up posters and sent drink coasters to clubs warning cocaine users to start with a small dose and to have naloxone, an opioid reversal drug, on hand to counter an overdose. They are handing out fentanyl testing strips that can be used to test cocaine and other drugs for fentanyl’s presence.
Multiple people died within hours from tainted cocaine in Long Island, N.Y., and in Newport Beach, Calif., last year. Nine were killed in Washington, D.C., in January. Law-enforcement officials said dealers often use coffee grinders or other basic equipment to cut drugs and prepare them for sale, which can result in deadly batches.
From the FEHB front, Tammy Flanagan, writing in Govexec, advises federal and postal employees and annuitants on how to prepare for the upcoming Federal Employee Benefits Open Season. The FEHBlog’s advice is to stack your plan’s summary of benefits and coverage which is available on all FEHB plan websites against other plans in which you are interested. The summary of benefits and coverage, which is an Affordable Care Act requirement, is four double-sided pages including consumer-tested practical information.
From the Omicron and siblings’ front
STAT News reports “FDA’s vaccines chief [Peter Marks, MD] sees the possibility of more Covid boosters — sooner than he’d like.”
Pfizer is considering hiking the price of its COVID-19 vaccine by roughly four times what it currently charges as it prepares for sales in the U.S. to shift from government contracts to the private market.
The pharmaceutical company is targeting between $110 and $130 per adult vaccine dose after that transition, said Angela Lukin, Pfizer’s head of global primary care and U.S. president, on an analyst and investor call Thursday.
“We feel confident that this range will be seen as highly cost effective and definitely one that will help to enable and ensure appropriate access and reimbursement to the vaccine,” Lukin said on the call. Discussions with insurers are still in early stages, she added.
No doubt this charming development seeks to pressure Congress to add more federal Covid dollars in the lame-duck session following the November 8 Congressional election.
In other vaccine news, MedPage Today reports
The CDC’s vaccine advisors updated their recommendations to clarify when to administer the 20-valent conjugate pneumococcal vaccine (PCV20; Prevnar 20) in adults who previously received the 13-valent conjugate vaccine (PCV13; Prevnar 13).
Three doses of hepatitis B vaccine with a cytosine phosphoguanine adjuvant (HepB-CpG; Heplisav-B) notched a perfect mark when it came to seroprotection for people with HIV who had never before been vaccinated against the hepatitis B virus (HBV), early results of a phase III trial showed.
In prescription drug development news, Fierce Healthcare points out “three drugs are set for FDA determinations soon.” The article explains why Optum says payers should take notice.
Cases of monkeypox are continuing to decline in the U.S., but the disease is still disproportionately affecting people of color, a White House official said.
“In the U.S., about 27,635 cases were reported as of yesterday,” Demetre Daskalakis, MD, White House National Monkeypox Response deputy coordinator, said at an online briefing Thursday. “We continue to have a decrease over time — we’re about 85% down from where we were at the peak of the outbreak. So that’s a lot of hopeful news, that we continue to see monkeypox going under better and better control.”
From the mental healthcare front, the Department of Health and Human Services “through the Substance Abuse and Mental Health Services Administration (SAMHSA), announced more than $100 million this week in funding from the Bipartisan Safer Communities Act (BSCA) to states and territories for mental health emergency preparedness, crisis response, and the expansion of 988 Suicide & Crisis Lifeline services. BSCA, signed into law by President Biden earlier this year, provided unprecedented funding to address the nation’s mental health crisis and make our communities safer.”
From the maternal care front, Health Payer Intelligence informs us Blue Cross and Blue Shield of Michigan has “decided to go beyond traditional maternal healthcare benefits, such as prenatal and postpartum care coverage. They teamed up with a virtual care provider for women and family health, Maven, to offer a suite of solutions that integrated family care and maternal healthcare.”
In a letter to HHS Secretary Xavier Becerra and Management and Budget Office Director Shalanda Young, AHIP explained its vision for how demographic data can be improved and standardized across the healthcare system.
Five things to know about the association’s recommendations for improving demographic data:
1. Current challenges with demographic data include the lack of specificity for questions on race. AHIP highlights that current census and HHS standards do not include an option for people to identify as Arab, Middle Eastern or North African. Additionally, AHIP recommends options should be tailored to the local area, depending on the populations that live there.
2. Current demographic questions do not have an “I choose not to respond” option. AHIP advises that a lack of information about how demographic information is used can lead to a lack of trust from patients.
3. Current regulations that require multiple providers and payers to collect demographic information lead to inconsistent results and greater burden on patients, AHIP says.
4. To reduce burdens on providers and patients, AHIP wants demographic data to be electronic and able to be shared with other places in the healthcare system with patient consent.
5. AHIP wants a wide range of government agencies to adopt its recommendations for demographic data collection, which include questions on race, ethnicity, language preference, sexual orientation, gender, diability status, veteran status and spirtual beliefs.
STAT New discusses weaknesses in traditional Medicare catastrophic coverage. FEHBlog suggests that Congress stop permitting Medicare supplemental plans to impose pre-existing condition limitations unless circumscribed by state law.
The Society for Human Resources Management tells us
Employee 401(k) contributions for 2023 will top off at $22,500—a $2,000 increase from the $20,500 cap for 2022—the IRS announced on Oct. 21. Plan participants age 50 or older next year can contribute an additional $7,500, up $1,000 from 2022. * * *
he limit on total employer-plus-employee contributions to defined contribution plans will increase to $66,000 in 2023, up by $5,000 from $61,000 in 2022. “This limit usually increases by $1,000 at a time but now it’s jumping five steps in one year,” Sit said.
The IRS announced the 2023 adjustments for 401(k) and similar defined contribution plans, and for defined benefit pension plan, in Notice 2022-55.
The American Hospital Association reports “The AHA and American Medical Association Oct. 19 filed a friend-of-the-court brief in support of a Texas Medical Association lawsuit claiming the revised independent dispute resolution process for determining payment for out-of-network services under the No Surprises Act skews the arbitration results in commercial insurers’ favor in ways that violate the compromise Congress reached in the Act.”
Business Insurance tells us “The U.S. Department of Justice has asked for more details on CVS Health Corp.’s proposed $8 billion deal to buy Signify Health, in a possible indication that the transaction will face a longer deal review rather than a quick approval, Reuters reports. The deal, announced last month, was expected to face a tough antitrust review even though the two companies do not compete directly in any market, according to experts.”
Following up on last Thursday’s post, RSV is a type of common cold according to the CDC.
Let’s lead off with the OPM Inspector General’s new annual report on top management challenges facing the agency. This is the first such report of the current Inspector General Krista Boyd. The report’s FEHB Program concerns focus on prescription drug spending, eligibility issues, and the Postal Service Health Benefits Program.
As the FEHBlog has noted, FEHB prescription drug spending is not a unique FEHB issue. While the Inspector General’s report calls attention to these statistics:
As in prior years, drug costs continue to increase in the FEHBP. Currently, total FEHBP drug costs (excluding drugs administered in an inpatient hospital setting) represent approximately 32 percent of total health care costs. Approximately 23 percent of total FEHBP health care costs are attributable to the pharmacy benefit alone (drugs dispensed through outpatient pharmacies). As of 2021, FEHBP pharmacy benefits represented more than $13 billion annually.
To place these statistics in context, the FEHB again calls attention to the fact that the FEHB Program has a large cadre of annuitants with primary Medicare Parts A and B coverage. This group understandably does not enroll for Medicare Part D prescription drug coverage. As a result, Medicare picks up the bulk of cost of FEHB hospital and doctor expenses for this group, while FEHB covers virtually of the pharmacy spending for this group. The FEHBlog is unaware of any other large employer in this situation because employers who have retiree health coverage generally rely on Medicare Advantage plans.
The saving grace found in Congress’s design of the FEHB Program is that all enrollees are in one risk pool per plan option which allows carriers to compete and also use group insurance principles to spread costs among all enrollees. Medicare prime annuitant and younger enrollees subsidize the more costly people in the middle.
The FEHBlog agrees with the Inspector General that the FEHB has eligility issues principally because OPM in contrast to every other employer in the U.S. reports enrollment and premiums separately. Typically health plans receive enrollment rosters known as HIPAA 820 standard electronic transactions that list each enrolled individual and the premium paid for that individual. This allows the health plan to systematically compare the roster and premiums against their records. A plan for example would know that OPM is paying it for self only coverage when according to the plan’s records the member has self plus one coverage.
OPM has been building a master enrollment index which is one of the steps that OPM has been taking in the right direction. In the FEHBlog’s opinion, implementing the HIPAA 820 standard transaction would take eligibility off of the Inspector General list of management challenges.
As for the Postal Service Health Benefits Program, the FEHBlog has confident that OPM, with support from the Postal Service and carriers, to launch the PSHBP on time January 1, 2025.
Here’s a Govexec article on the report which takes a broader perspective.
From Omicron and siblings front —
STAT News reports on the federal government’s and drug manufactures efforts to close the developing treatment gap for immunocompromised folks who contract certain strains for Omicron, e.g., BA 4.2.y and BQ.1
[Monoclonal antibody] Evusheld is still effective against many variants, but it is not possible for physicians to know which strains a patient using it as prophylaxis could be exposed to, an AstraZeneca spokesperson told STAT.
“Variants are rarely dominant for more than a few months — they tend to either evolve further into different subvariants or are replaced by newer variants,” the spokesperson said, adding the company is running early studies on other antibody options. * * *
Complicating the matter, the next potential monoclonal antibody — an Eli Lilly treatment dubbed bebtelovimab — could be ready within two months, but it has already been shown ineffective against the other fast-rising variant, BQ.1. The federal government has purchased 60,000 bebtelovimab doses for uninsured and under-insured patients, according to two people familiar with the HHS monoclonal antibody planning.
In the HHS meeting, officials discussed the prospect that BA.4.6’s rise could render Evusheld ineffective within two months. They laid out the timelines for as many as six potential alternates in the pipeline, according to two people familiar with the discussion.
a new national biodefense strategy, aiming to adapt lessons drawn from the rocky response to the Covid-19 pandemic as it prepares the country for future public health emergencies.
The strategy, which has been long anticipated, includes such goals as strengthening public health workforces both in the United States and globally, and establishing international mechanisms to bolster laboratory safety.
The government’s plan outlines policy targets for more than 20 federal agencies to help the country and world try to prevent epidemics, detect them faster, respond when they occur, minimize their impact, and recover, senior administration officials said on a call with reporters Monday as they previewed the strategy. Oversight for the strategy will be at the White House, under the national security advisor.
On a related note, Insurance News Net discusses the pandemic’s adverse impact on the life insurance industry, and Healthcare Dive tells us “The HHS’ current management of the strategic national stockpile and its subsequent relaying of information to Congress is fractured and needs updates to ensure the country is prepared for future public health emergencies, according to a report from the Government Accountability Office.”
From the SDOH front, MedPage Today delves into a CDC Vital Signs reports released yesterday
Influenza-associated hospitalization rates were nearly 80% higher among Black adults compared with white adults from 2009-2010 to 2021-2022, according to a CDC Vital Signs report released Tuesday.
These rates were also 30% higher among American Indian/Alaska Native (AI/AN) adults and 20% higher among Hispanic adults compared with white adults, reported Carla L. Black, PhD, of the CDC’s National Center for Immunization and Respiratory Diseases, and colleagues.
Furthermore, vaccination coverage for influenza has been “consistently lower among Black, Hispanic, and American Indian and Alaska Native adults since 2010,” she noted on a call with reporters.
During the 2021-2022 flu season, vaccination coverage was lower among Hispanic (37.9%), AI/AN (40.9%), Black (42.0%), and other/multiple race (42.6%) adults compared with coverage among white (53.9%) and Asian (54.2%) adults, Black and team said.
From the IRS front, the Service issued its annual notice of inflation adjustments to tax items for the 2023 tax year. The Wall Street Journal adds “The Internal Revenue Service adjusted key tax code parameters for 2023 to reflect higher inflation, raising the standard deduction and the income thresholds where tax rates take effect.” The notice also includes many inflation adjustments to tax-exempt or deductible employees benefits. You will find a handy table of contents at the front of the notice.
From the miscellany department
The Justice Department on the Food and Drug Administration’s behalf has asked various federal courts to shut down the e-cigarette operations of six manufacturers.
The Justice Department also announced Sutter Health’s agreement “to pay $13 million to settle allegations that it billed government health programs for lab tests performed by others,” said U.S. Attorney Stephanie M. Hinds. ‘Government health care programs [including the FEHB in this case] must be protected, and this office will investigate and pursue health care providers that fail to provide the services paid for by public health care programs.’”
Apple will reportedly enter the health insurance business in 2024 in partnership with a major payer, Forbes reported Oct. 18.
CCS Insight’s chief analyst predicts the tech giant will power the new offering through health data collected by Apple Watches, such as blood pressure, blood oxygen levels, ECG readings and body temperature. The analyst said having access to this data from the beginning gives the company an advantage toward entering the market and cutting costs.
Reg Jones writing in the Federal Times explains how to enroll for Medicare Part without incurring a late enrollment penalty. It’s not hard if you know the rules.
Fortune Well considers a change in the spread of Omicron. “COVID has splintered into multiple variants dominating different countries at the same time. Experts say these are some scenarios could play out.”
The American Medical Association answers patient FAQs about the upcoming winter in which Covid is not expected to eclipse the flu.
The FDA encourages Americans, including children, to get the flu vaccine.
Fortune Well provides advice on who is a candidate for the monkeypox vaccine now that this vaccine is more widely available.
The Bill and Melinda Gates Foundation says it will commit $1.2 billion to the effort to end polio worldwide.
The money will be used to help implement the Global Polio Eradication Initiative’s strategy through 2026. The initiative is trying to end the polio virus in Pakistan and Afghanistan, the last two endemic countries, the foundation said in a statement Sunday.
The money also will be used to stop outbreaks of new variants of the virus. The announcement was made Sunday at the World Health Summit in Berlin.
The foundation says in a statement on its website that it has contributed nearly $5 billion to the polio eradication initiative. The initiative is trying to integrate polio campaigns into broader health services, while it scales up use of the novel oral polio vaccine type 2.
The group also is working to make national health systems stronger so countries are better prepared for future health threats, the statement said.
From the price transparency front, two consultants from the Berkley Research Group advise in Healthcare Dive
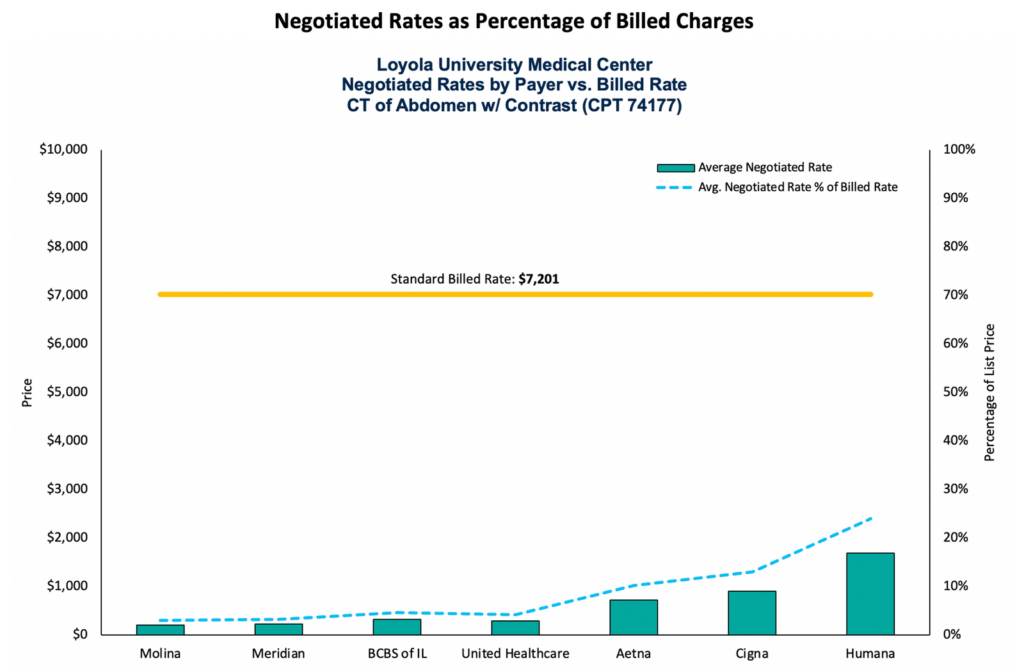
Payers can use hospital transparency data to gain insights regarding the rates hospitals have negotiated with other payers, which potentially can be used during contract negotiations. For example, payers can evaluate the negotiated rates for specific hospitals compared to their competitor health plans to gauge alignment with their proposed rates and discounts. This is illustrated in Figure 2, which shows the average negotiated rates for a CT scan of the abdomen (CPT 74177) for each payer who contracts with Loyola University Medical Center near Chicago, compared to the hospital’s standard billed charge for the procedure. As shown in the graph, the average negotiated rate as a percentage of billed charges (list price) ranges from 3% to 24% (about $200 to $1,800).
The article offers other approaches to using hospital transparency data, e.g., geographic methods.
CVS Health wants to be in charge of the “entire spectrum of someone’s health journey,” the company’s chief executive said at an Oct. 12 event in Boston reported on by the Boston Business Journal.
CEO Karen Lynch pointed to how the company already delivers medication at the pharmacy, finances treatments through insurance company Aetna, provides low-cost urgent care at its MinuteClinics, and now intends to give care at home through its planned $8 billion acquisition of Signify Health, she reportedly said at the Boston College Chief Executives Club meeting.
Ms. Lynch said the company also plans to expand into primary care and expects to announce an acquisition later this year, the Business Journal reported Oct. 13. CVS is rumored to be in exclusive talksto buy Cano Health, a primary care firm focused on seniors.
Ms. Lynch told the crowd CVS has advantages over fellow healthcare disruptor Amazon, which recently agreed to acquire primary care chain One Medical for $3.9 billion, according to the story. “[Customers] really want to trust and engage with companies that have earned the right to be in healthcare,” she said. “I think about Amazon as sort of a transactional company today.”
The American Hospital Association informs us
President Biden today directed the Center for Medicare and Medicaid Innovation to consider new payment and delivery models to lower drug costs and promote access to innovative drug therapies for beneficiaries, and report within 90 days on its plan and timeline for testing selected models. AHA will update members as more information on the plan becomes available.
The White House also released a fact sheet on this executive order.
The American Medical Association issued a research report titled “Competition in Commercial PBM Markets and Vertical Integration of Health Insurers with PBMs.” The report is chock-a-block full of various PBM rankings.
Speaking of the CMS innovation center, the American Hospital Association reports
The Centers for Medicare & Medicaid Services will extend through 2025 the Bundled Payments for Care Improvement Advanced model, which was set to expire this year. CMS launched the alternative payment model in 2018 to test whether bundling Medicare payments for certain inpatient and outpatient care reduces spending and improves quality. The agency expects early next year to request applications from Medicare providers, suppliers and accountable care organizations to participate in the two-year extension, which will include changes to the pricing methodology.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.