Thursday Miscellany

From Capitol Hill, the Wall Street Journal reports that the Senate majority’s leadership is rallying the caucus to pass the Schumer – Manchin compromise reconciliation bill that would address climate and healthcare concerns while raising taxes. The goal is for the Senate to pass the bill next week which immediately precedes the Senate’s August recess.
The Hill adds that
A day after Sen. Joe Manchin (D-W.Va.) stunned Washington by endorsing hundreds of billions of dollars for President Biden’s domestic agenda, House Democrats are rallying behind the nascent package as a crucial — if incomplete — strategy for tackling the climate crisis and easing working class economic strains.
Both articles discuss the flies remain in the reconciliation ointment.
Govexec informs us
The odds that Congress would increase the average 4.6% pay raise planned for federal employees in 2023 got a little longer Thursday, after Senate appropriators revealed that they would effectively endorse President Biden’s pay increase proposal.” The Senate Appropriations Committee on Thursday revealed all of their initial versions of fiscal 2023 spending bills, including the package governing financial services and general government, which is the vehicle by which Congress weighs in on federal employee compensation. That bill makes no mention of changes to career federal employees’ pay, effectively endorsing the pay raise plan offered by Biden in his fiscal 2023 budget proposal.
Here is a link to the Senate Appropriations Committee’s press release unveiling those bills. What caught the FEHBlog’s eye is the statement in the press release that the Senate appropriations bills, like the House appropriations bills, do not include the Hyde amendments limiting federal funding of abortions to cases of rape, incest, or endangerment of the mother’s life. That tectonic change would draw the FEHBP into the post-Dobbs controversy.
From the Affordable Care Act front, Prof. Katie Keith does her usual outstanding job breaking down the proposed ACA Section 1557 individual non-discrimination rule in Health Affairs Forefront. In the FEHBlog’s view, the rule is unnecessarily complicated. It is the FEHBlog’s understanding that this HHS rule would not apply to FEHBP and that HHS would refer Section 1557 complaints involving FEHB plans to OPM. As the preamble points out, Section 1557 is a law that doesn’t need an implementing rule. Nevertheless, HHS recommends that other agencies with programs covered by Section 1557 adopt their own implementing rule using the HHS rule as a template.
The ACA regulators issued a 13-page long ACA FAQ 54 describing in detail the ACA rule requirements under which health plans must cover contraceptive drugs and services for women without cost sharing.
On a related note, Healthcare Dive tells us
Melanie Fontes Rainer is now acting director of HHS’ Office of Civil Rights. Fontes Rainer will replace Lisa Pino, who oversaw rulemaking related to patient safety, reproductive rights and other healthcare issues and issued policy regarding health equity, long COVID and firearm injury and death prevention, the agency said in an emailed statement.
From the federal employee benefits front, Fedweek explains the circumstances under which survivors of federal employees (as opposed to federal annuitants) are eligible for federal survivor benefits.
If you are an employee who was married when you die and you had at least 18 months of creditable civilian service, your spouse will be entitled to a survivor annuity. * * * f you were enrolled in either the self plus one or self and family options of the Federal Employees Health Benefits program when you died, the person(s) on your enrollment could continue that coverage. If you weren’t enrolled in the program (or were enrolled but in the self only option), any otherwise eligible survivors would be out of luck.
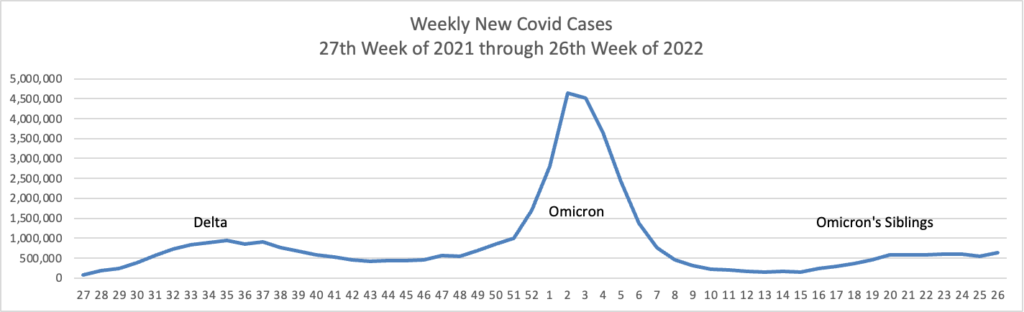
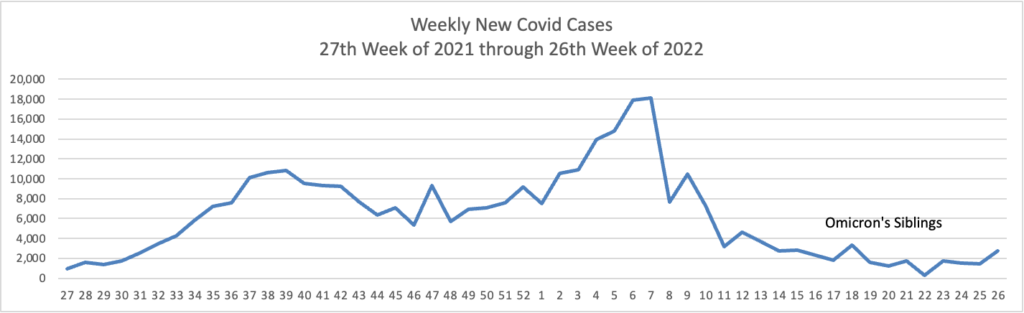
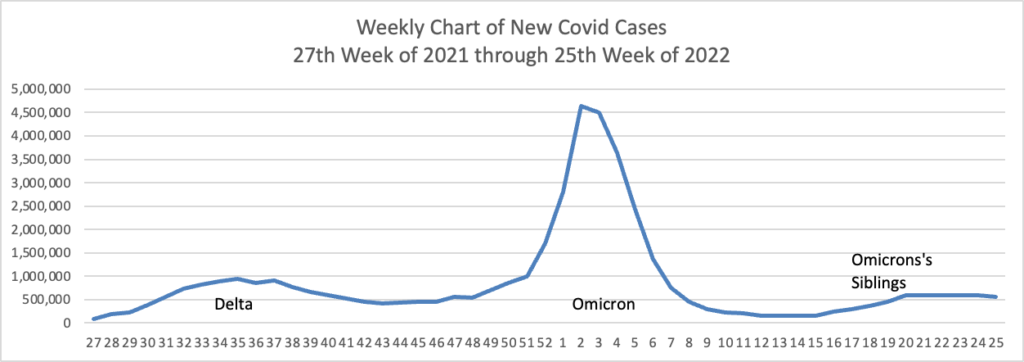
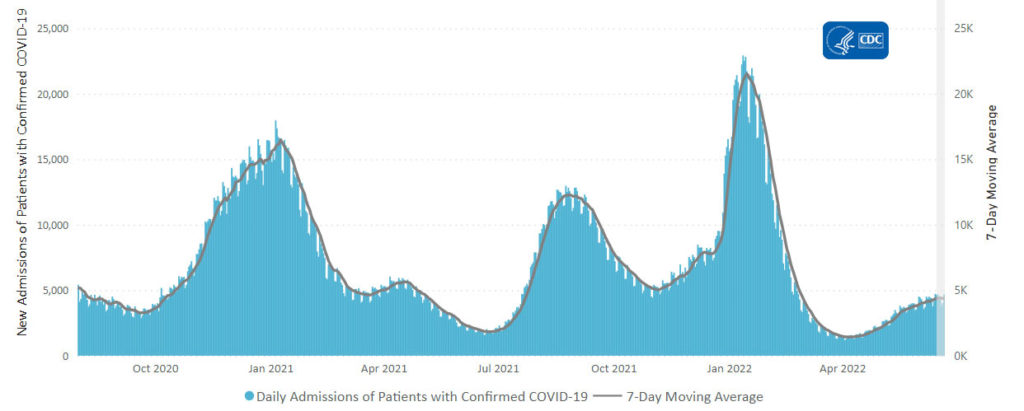
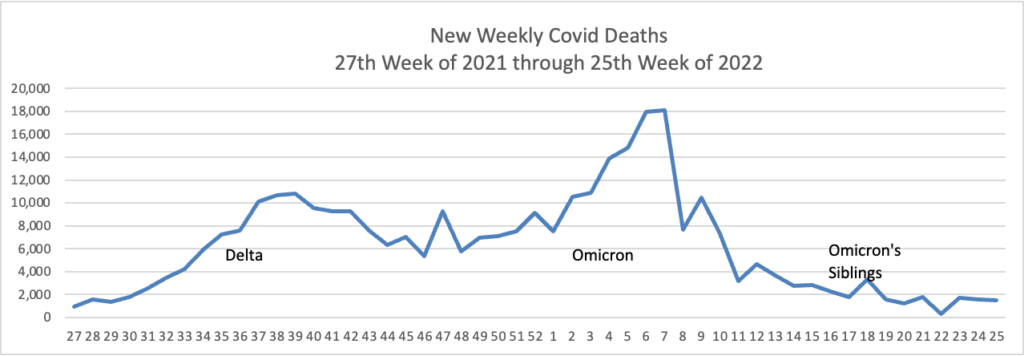
From the Omicron and siblings front, the American Medical Association offers a helpful Q&A on Covid boosters.
From the monkeypox front, Reuters makes two reports
- The United States has the capacity to conduct 60,000-80,000 tests for monkeypox virus per week, Health and Human Services Secretary Xavier Becerra said on Thursday. When the monkeypox outbreak began, the U.S. was able to conduct only 6,000 tests per week, Becerra told reporters during a telephone briefing.
- The U.S. Centers for Disease Control and Prevention (CDC) said on Wednesday it plans to make the rapidly spreading monkeypox disease a nationally notifiable condition. The designation, which is set to take effect on Aug. 1, updates criteria for reporting of data on cases by states to the agency and would allow the agency to monitor and respond to monkeypox even after the current outbreak recedes, the CDC said.
From the U.S. healthcare business front —
The American Hospital Association issued a report attacking the commercial health insurance industry, which in the FEHBlog’s view is akin to strangling the golden goose.
Healthcare Dive reports
Teladoc beat Wall Street expectations for revenue in the second quarter, with a topline of $592 million, up 18% year over year. Chronic care membership came in higher than analysts expected, while member utilization improved year over year.
But “all eyes” are on the vendor’s guidance for the rest of the year, which implies a third-quarter miss and a steep ramp-up for earnings in the fourth quarter, SVB Securities analyst Stephanie Davis wrote in a note on the results.
STAT News chimes in
Telehealth giant Teladoc is bracing for disappointing earnings this year as it faces headwinds that could also thwart competitors struggling to turn a profit — including increasingly frugal employers delaying or dropping contracts for virtual care.
“The challenge that we’re seeing is in these times of economic uncertainty, all purchases are just getting a significantly higher level of scrutiny,” CEO Jason Gorevic said in an earnings call Wednesday.
Gorevic also noted that declining yield on advertising suggests that individual patients may start spending less on direct-to-consumer services like BetterHelp, the company’s mental health care offering. Those hurdles aren’t unique to Teladoc. Competitors like Amwell and Talkspace could also have to grapple with cutbacks.
Healthcare Dive also delves into Amazon’s planned acquisition of One Medical. “The deal fast-tracks Amazon’s ambitions in healthcare, while giving One Medical a cushion in today’s tricky economic environment.”
Yesterday, the FEHB wrote about the hospitals receiving five stars from Medicare. Today Becker’s Hospital Review lists the 192 hospitals receiving a single start from that program.
Finally STAT News lists the 41 best books and podcasts on health and science to check out this Summer.