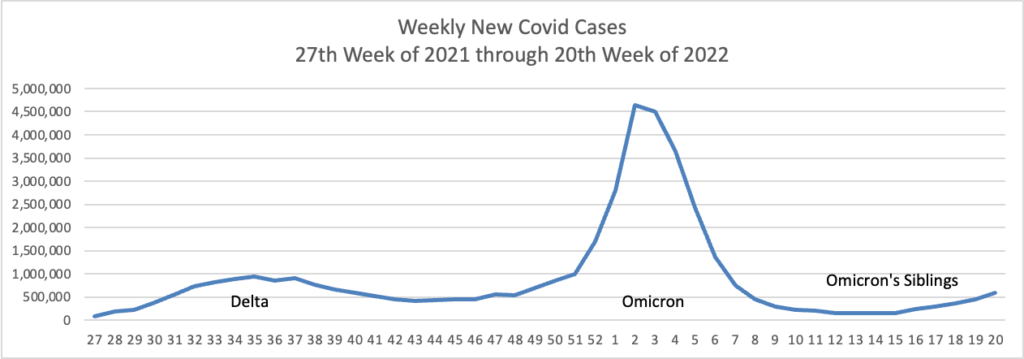
Based on the CDC’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s weekly chart of new Covid cases from the 27th week of 2021 through the 20th week of 2022:
The CDC’s weekly review of its COVID statistics notes
As of May 18, 2022, the current 7-day moving average of daily new cases (101,130) increased by 18.8% compared with the previous 7-day moving average (85,143). A total of 82,820,565 COVID-19 cases have been reported in the United States as of May 18, 2022.
Here is the CDC’s chart seven-day movings averages of new Covid hospital admissions:
The CDC’s weekly review notes “The current 7-day daily average [of new hospital admissions for Covid] for May 11–17, 2022, was 3,250. This is a 24.2% increase from the prior 7-day average (2,617) from May 4–10, 2022.
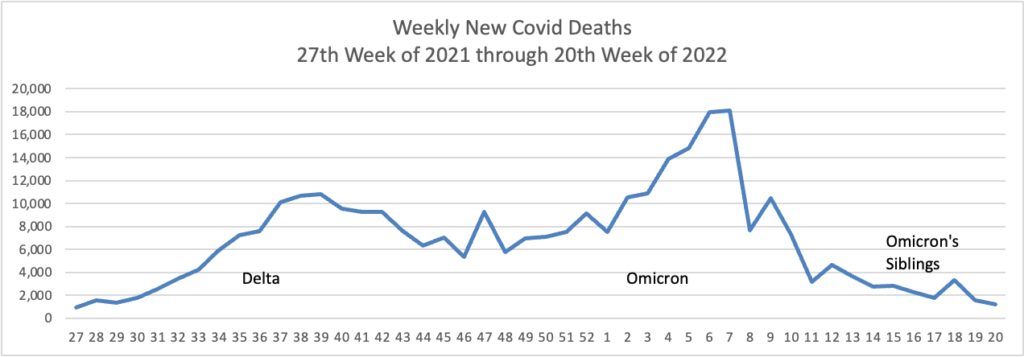
Here’s the FEHBlog’s weekly chart of new Covid deaths over the same period as the new weekly cases chart:
The CDC’s weekly review notes:
The current 7-day moving average of new deaths (280) has decreased 1.2% compared with the previous 7-day moving average (284). As of May 18, 2022, a total of 998,512 COVID-19 deaths have been reported in the United States.
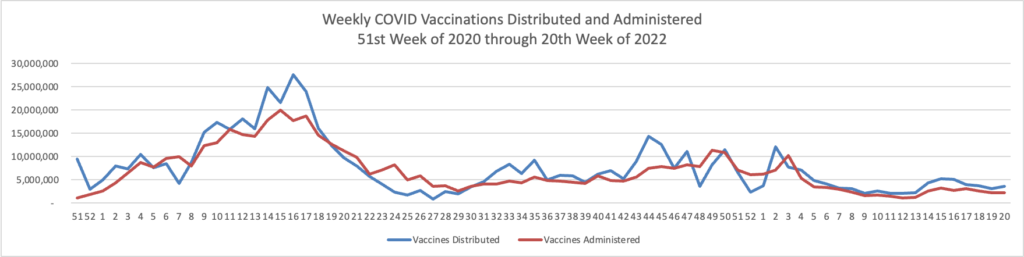
Here’s the FEHBlog’s weekly chart of Covid vaccinations distributed and administered from the beginning of the Covid vaccination program in December 2020 through the 20th week of 2022.
The CDC’s weekly review notes “As of May 18, 2022, the 7-day average number of administered vaccine doses reported (by date of CDC report) to CDC per day was 388,308, a 0.5% decrease from the previous week.”
To sum it up, the CDC’s weekly review points out,
As of May 19, 2022, there are 301 (9.35%) counties, districts, or territories with a high COVID-19 Community Level, 477 (14.81%) counties with a medium Community Level, and 2,442 (75.84%) counties with a low Community Level. This represents a moderate (+5.10 percentage points) increase in the number of high-level counties, a slight (−0.74 percentage points) decrease in the number of medium-level counties, and a corresponding (−5.84 percentage points) decrease in the number of low-level counties. Five (9.62%) of 52 jurisdictions had no high- or medium-level counties this week.
Federal News Network suggests “Federal employees [and annuitants] can use these next few months between now and open season, which begins Nov. 14, to do something that most feds rarely do — research and planning [for Open Season]. The article suggests how to conduct this research, and the FEHBlog thinks that Federal News Network is on the right track.
A growing number of Senate Democrats say they’re ready to take a tough vote on an amendment to keep the Title 42 health order in place at the U.S.-Mexico border if that’s what’s needed to move a stalled COVID-19 relief package.
Senate Majority Leader Charles Schumer (D-N.Y.) has held the bill from the floor because Republicans are insisting on voting on a bipartisan amendment to overrule the Biden administration’s decision to lift Title 42, a pandemic order that has stopped thousands of immigrants from entering the country on asylum claims. * * *
Without giving in to the Republicans’ demand for a vote on the hot-button issue of securing the border, COVID-19 relief could be stalled until after the November election.
The amendment is expected to fail but it’s a tough vote for vulnerable Senate Democrats.
More likely, in the FEHBlog’s view, the Majority Leader is waiting until the Title 42 health order is lifted later this month to see what happens.
Following the recommendation Thursday, many of the nation’s doctors, pharmacies and other vaccination sites are expected to begin offering the extra doses to the 28 million U.S. children in the age group.
The shots are to be given five months after the second dose. The extra dose is one-third the amount that those 12 years old and above receive.
Also Thursday, the CDC said it was strengthening its recommendation that people 12 years and older who are immunocompromised, or who are 50 and older, should receive a second booster dose at least four months after their first.
This means that health plans must start covering the booster with no member cost-sharing pursuant to ACA FAQ 50.
“We are ready from a manufacturing standpoint,” Moderna Chief Executive Stéphane Bancel said during a virtual appearance Thursday at The Wall Street Journal’s Future of Everything Festival.
The FDA/CDC decision is expected next month.
In other virus news, STAT News interviewed a top CDC expert on monkeypox. From the FEHBlog’s standpoint, the key takeaway is that monkeypox is not Covid.
I think we can take away a lot from what we know about monkeypox in Congo Basin and in West Africa. Even if human-to-human transmission is documented, it is generally documented among very close contacts. So family members, people taking care of ill patients. Or health care providers.
In funding news, the Department of Health and Human Services announced today a $1.5 billion funding opportunity under the State Opioid Response
SOR grant program provides formula funding to states and territories for increasing access to FDA-approved medications for the treatment of Opioid Use Disorder (OUD), and for supporting prevention, harm reduction, treatment, and recovery support services for OUD and other concurrent substance use disorders (SUD). The SOR program also supports care for stimulant misuse and use disorders, including for cocaine and methamphetamine. The SOR program helps reduce overdose deaths and close the gap in treatment needs across America by giving states and territories flexibility in funding evidence-based practices and supports across different settings to meet local community needs.
From the miscellany department
Today “the U.S. Office of Personnel Management (OPM) released guidance regarding the implementation of EO 13932; Modernizing and Reforming the Assessment and Hiring of Federal Job Candidates. OPM’s guidance represents a major step towards the federal government’s adoption of skills-based hiring practices and is an important innovation in federal hiring, which has historically relied on education and candidate self-assessments as a proxy for a candidate’s ability to perform in a job. This new approach helps hiring managers recognize and value skills regardless of where they were acquired, whether in a formal degree program, on the job, or on one’s own.”
Employee Benefit News identifies the ten most popular mental health and wellness apps.
Benefits consultant Tammy Flanagan discusses federal employee life insurance benefits in Govexec.
Health Payer Intelligence reports that CMS has updated the Medicare.gov website “to include new features such as highlighting pages that answer popular questions and spotlighting key steps that consumers should take related to Medicare coverage.”
The seven-day moving average of new Covid-19 cases recently topped 94,000 a day, Centers for Disease Control and Prevention data show, nearly four times lows reached in late March. The true number of new cases is likely significantly higher, epidemiologists say, because so many people are self-testing at home or not testing at all.
The rise in cases hasn’t translated thus far into major surges in severe illness. The seven-day average of confirmed cases in hospitalized patients reached about 18,550 on Wednesday, up from lows near 10,000 in mid-April, but far below a record peak above 150,000 in January. The numbers include people who test positive on routine screening after getting hospitalized for other reasons. The daily average of reported deaths has slipped under 300 a day, the lowest point since last summer.
But * * * the more an outbreak spreads, the more likely it will reach the most vulnerable including elderly people and others with compromised immune systems, the experts say, and the more likely the virus will continue to mutate.
As Covid-19 again surges across the US, many people are going without time-sensitive therapeutics like Paxlovid because doctors worried about shortages are reluctant to prescribe the drugs. But the situation has changed and supplies are now abundant.
The Food and Drug Administration has issued emergency-use authorizations for the drug to treat mild to moderate Covid-19 in people who are at high risk. The Centers for Disease Control and Prevention defines those as individuals ages 50 years or older, unvaccinated, or with certain medical conditions like kidney, liver, lung and heart disease, diabetes, cancer and HIV. It also recommends the drug for people who are immunocompromised, pregnant, obese, cigarette smokers or suffering from mood disorders.
You can find the one stop test to treat locations “by using the Department of Health and Human Services’ Test to Treat Locator or by calling 1-800-232-0233.”
Kaiser Health News recommends “improving ventilation and filtration of the air. ‘Ventilation matters a lot,’ said Dr. Amy Barczak, an assistant professor of medicine at Harvard Medical School. ‘If you’re taking care of someone at home, it’s really important to maximize all the interventions that work.’”
Viral particles float through the air like invisible secondhand smoke, diffusing as they travel. Outside the home, viruses are quickly dispersed by the wind. Inside, germs can build up, like clouds of thick cigarette smoke, increasing the risk of inhaling the virus.
The best strategy for avoiding the virus is to make your indoor environment as much like the outdoors as possible.
In related viral news, Beckers Hospital Review tells us
More than 400 children worldwide have developed unusual cases of acute hepatitis, and researchers are still searching for the cause of the outbreak, the World Health Organization said May 17.
As of May 15, the WHO reported 429 probable cases in 22 countries, up from 348 cases a week prior, according to Philippa Easterbrook, MD, a senior scientist in the global hepatitis program at the WHO. Another 40 cases are still under investigation, and 75 percent of all affected children are under age 5.
Twelve countries are reporting more than five cases, double the amount from last week. Of these 12 countries, nine are in Europe. In total, six children have died in the outbreak and 26 have required liver transplants, according to Dr. Easterbrook.
As of May 17, researchers were still investigating the cause of the hepatitis outbreak. The leading hypothesis is that an adenovirus and SARS-CoV-2, the virus that causes COVID-19, may be causing hepatitis in children. Scientists are exploring “how these two infections may be working together as co-factors either by enhancing susceptibility or creating an abnormal response,” Dr. Easterbrook said.
From the healthcare policy front, AHIP today launched
Healthier People through Healthier Markets, a new policy roadmap and set of solutions to improve health care affordability and access for every American. The effort is focused on boosting competition in health care markets and reining in harmful practices that hurt American families. With the launch of this policy roadmap, AHIP sent letters to President Biden and the leadership of Congress that lay out a detailed set of legislative and regulatory enforcement actions to increase competition in health care, drive down costs, and improve health care access for patients.
The Office of Personnel Management on Wednesday urged federal agencies to ensure their employees are aware and can access the mental health benefits provided to federal workers, in light of May being Mental Health Awareness Month.
In a memo to agency heads, OPM Director Kiran Ahuja noted that promoting the federal workforce’s wellbeing, including mental health, is a priority in President Biden’s management agenda.
“We want to make sure that all federal employees understand the supports available to them and underscore that there should be no shame or stigma for taking care of their mental health,” Ahuja wrote. “[As] a reminder, employee assistance programs and Federal Employees Health Benefits health plans offer mental health services to employees and their family members. We encourage agencies to proactively communicate to their workforces about their options and encourage employees to contact their agency benefits officers or EAP coordinator to learn more.”
The FEHBlog encourages OPM to better coordinate mental health care services among FEHB plans, EAPs and wellness programs.
mHealth Intelligence informs us “In the second half of 2020, only 14.1 percent of children used telehealth due to the pandemic, but use was higher among those with asthma, a developmental condition, or a disability, the Centers for Disease Control and Prevention (CDC) found.”
From the survey department, Beckers Payer Issues advises that “Castlight Health analyzed more than 160 million commercial medical claims nationwide to reveal insights about healthcare utilization patterns from 2018 to 2021.” Castlights report ranks the fifty States and DC based on average medical spending per member in 2021.
From the miscellany department —
Beckers Payer Issues reports “Anthem shareholders voted at their annual meeting May 18 to change the company’s name to Elevance Health.”
Federal News Network discusses the Postmaster General’s plans to close and consolidate Postal facilities across the delivery network. “The network transformation initiative will impact nearly 500 network mail processing locations, 1,000 transfer hubs and 100,000 carrier routes. It will also impact 10,000 delivery units, which USPS defines as post offices, stations, branches or carrier annexes that handle mail delivery functions.”
FedSmith tells us “Starting May 26, 2022, federal retirees will notice a new process for signing into the OPM Retirement Services Online website. The login process will now be managed through the federal government’s Login.gov website and will require you to create a new username and password at login.gov if you do not currently have one.”
The Wall Street Journal has updated its article on Covid boosters.
The Institute for Clinical and Economic Review (ICER) today released “a Final Evidence Report assessing the comparative clinical effectiveness and value of [specific] outpatient treatments for COVID-19 [, principally Pfizer’s pill Paxlovid and Merck’s pill molnupiravir ].
A majority (11-2) found current evidence is notadequate to demonstrate a net health benefit when molnupiravir is compared to symptomatic care alone.
All panelists (13-0) found that current evidence is adequate to demonstrate a net health benefit when Paxlovid is compared to symptomatic care alone.
Due to uncertainty in the net health benefit for molnupiravir, a majority of panelists voted that it represents “low-to-intermediate” long-term value for money.
A majority of panelists found that Paxlovid represents “high” long-term value for money.
ICER presented at the OPM/AHIP carrier conference last month. ICER “is an independent non-profit research institute that produces reports analyzing the evidence on the effectiveness and value of drugs and other medical services. ICER’s reports include evidence-based calculations of prices for new drugs that accurately reflect the degree of improvement expected in long-term patient outcomes, while also highlighting price levels that might contribute to unaffordable short-term cost growth for the overall health care system.”
Speaking of the Covid pills, STAT News discusses the use of telehealth services to prescribe them. The upshot, as the FEHBlog understands it, is while using telehealth for this purpose is convenient for patients, experts are unsure whether the telehealth service provides adequate follow-up care to the patient.
Also, from the Rx coverage front, the Food and Drug Administration issued a news roundup today.
From the healthcare business front, BioPharma Dive reports
Pfizer has agreed to acquire Biohaven Pharmaceuticals for $11.6 billion in a deal that turns an existing alliance on a fast-selling migraine drug into a big bet on its future growth.
Pfizer will pay $148.50 per share in cash for each Biohaven share it doesn’t already own, representing a roughly 79% premium to the company’s Monday closing price and a 33% premium to its average share price of $111.70 over the last three months. The deal, which is expected to close early next year, is by far the biggest biotech buyout of 2022, according to data compiled by Biopharma Dive.
Announced Tuesday, the acquisition hands Pfizer full rights to Nurtec ODT, a pill that’s approved in the U.S. and other countries for the treatment and prevention of migraines. Biohaven’s pipeline also includes an experimental nasal spray for migraines, zavepegant, that’s been submitted to U.S. regulators, as well as five additional, preclinical treatments that block the same protein target.
From the mental health parity front, the Labor Department’s Employee Benefits Security Administration announced that the agency will be holding a mental health parity compliance assistance webcast on May 24 from 2-3 pm ET. Here is a link to the announcement which explains how to register for the webcast.
From the patient safety front, the Leapfrog Group “released the spring 2022 Leapfrog Hospital Safety Grade, which assigns a letter grade to nearly 3,000 U.S. general hospitals based on over 30 measures of patient safety.”
At HospitalSafetyGrade.org, the public can find detailed information about a hospital’s performance on patient experience and other safety measures used to grade hospitals.
Across all states, highlights of findings from the spring 2022 Leapfrog Hospital Safety Grade include:
Thirty‐three percent of hospitals received an “A,” 24% received a “B,” 36% received a “C,” 7% received a “D,” and less than 1% received an “F.”
Five states with the highest percentages of “A” hospitals are North Carolina, Virginia, Utah, Colorado, and Michigan.
There were no “A” hospitals in Wyoming, West Virginia, the District of Columbia, or North Dakota.
From the medical research department, Medscape informs us
Eight modifiable risk factors were linked to more than one in three cases of Alzheimer’s disease and related dementia in the U.S., a cross-sectional analysis showed.
The eight risk factors — midlife obesity, midlife hypertension, physical inactivity, depression, smoking, low education, diabetes, and hearing loss — were associated with 36.9% (95% CI 36.5-37.3) of Alzheimer’s and dementia cases, reported Roch Nianogo, MD, PhD, of the University of California Los Angeles, and Deborah Barnes, PhD, MPH, of the University of California San Francisco, and co-authors.
The factors most prominently associated with Alzheimer’s and dementia were midlife obesity, at 17.7% (95% [Confidence Interval] CI 17.5-18.0); physical inactivity, at 11.8% (95% CI 11.7-11.9); and low educational attainment, at 11.7% (95% CI 11.5-12.0).
“We published a similar study a little more than 10 years ago, and the most important risk factors then were physical inactivity, depression, and smoking,” Barnes told MedPage Today.
“Today, the top three risk factors are midlife obesity, physical inactivity, and low education,” she observed. “This is important because it suggests that the growing number of people who are obese in the U.S. could have a major long-term impact on dementia rates.”
From the clarification front, the FEHBlog often reminds folks that federal employees who retired under the Civil Service Retirement System before 1984 are not eligible for free Medicare Part A. The FEHBlog dug into this issue today, and he discovered this 2013 Reg Jones Q&A on this topic that the Federal Times published.
Q. I retired in 2009 under CSRS. I am close to 65, and the answer to one of the questions asked states that people in CSRS are not eligible for Medicare because they didn’t pay into Social Security.
I was in CSRS before the change to FERS and stayed with CSRS. I had Medicare deductions taken from my pay from 1983-84 till I retired in 2009.
Do the Medicare funds I paid since 1983 make me eligible for Medicare or just part of it?
So which is right? I need to know so I can do what needs to be done — enroll or not. I’m currently insured under federal BCBS.
A. CSRS employees who retired before Dec. 31, 1983, aren’t eligible for Medicare Part A. Nor are CSRS employees who retired after that date but before having Medicare deductions taken from their pay for 10 years.
On the other hand, they are eligible to enroll in Medicare Part B, which is open to everyone 65 or older.
Consequently, the cadre of 65 and older federal annuitants without Medicare A is larger than the FEHBlog understood. This cadre is relevant to the Postal Reform Act because that law keeps Postal annuitants over aged 65 without Medicare Part in the legacy FEHBP.
President Joe Biden and top Democrats have agreed to a GOP demand to disentangle a stalled COVID-19 response package from a separate supplemental request for military and humanitarian aid to Ukraine so the latter can move more quickly. * * *
Senate Minority Leader Mitch McConnell didn’t reject the outlines of the Democrats’ offer in brief remarks Monday. “It may adjust some in the process, but we need to do it quickly,” McConnell told Punchbowl, while adding he was pleased that COVID-19 funds and an immigration-related dispute that tangled up the pandemic relief bill would be handled separately.
A separate, bipartisan $10 billion aid package for the ongoing pandemic response effort has been held up for a month due to a dispute over the so-called Title 42 program that allows migrants to be turned away at the border to prevent the spread of COVID-19. Biden has proposed to end the Trump-era program as of May 23, which Republicans and several Senate Democrats have said they oppose without alternatives in place to stem the expected surge of migrants.
From the Omicron and siblings front, the Centers for Disease Control has updated its long Covid website. The CDC explains
What You Need to Know
Post-COVID conditions can include a wide range of ongoing health problems; these conditions can last weeks, months, or years.
Post-COVID conditions are found more often in people who had severe COVID-19 illness, but anyone who has been infected with the virus that causes COVID-19 can experience post-COVID conditions, even people who had mild illness or no symptoms from COVID-19.
People who are not vaccinated against COVID-19 and become infected may also be at higher risk of developing post-COVID conditions compared to people who were vaccinated and had breakthrough infections.
There is no single test for post-COVID conditions. While most people with post-COVID conditions have evidence of infection or COVID-19 illness, in some cases, a person with post-COVID conditions may not have tested positive for the virus or known they were infected.
CDC and partners are working to understand more about who experiences post-COVID conditions and why, including whether groups disproportionately impacted by COVID-19 are at higher risk.
Widely used physician guidelines that ignore patients’ race and ethnicity could be doing more harm than good when it comes to catching diabetes in people of color. New research, published in the Annals of Internal Medicine on Monday, suggests that people from certain racial and ethnic groups should be screened for diabetes at lower body mass index than non-Hispanic white people — a recommendation that contradicts recent guidelines from the United States Preventive Services Task Force.
It’s an admittedly tricky proposition, to reaffirm the role of race and ethnicity at a time when medicine is trying to rid itself of race-based tools — such as an algorithm used to assess kidney function — that have contributed to the large health disparities in the United States. The paper’s authors recognized as much in interviews with STAT.
They argue, however, that using a one-size-fits-all approach to screening, when diabetes is two to four times more prevalent and more deadly in Black, Hispanic, and Asian Americans, is likely to result in underdiagnosis of the disease, and widen health gaps.
From the healthcare business front, Fierce Healthcare informs us
Telehealth giant Amwell saw telehealth visits grow to 1.8 million in the first quarter of 2022, up 16% compared to the tail end of 2021 and up about 11% from 1.6 million virtual care visits during the same time last year.
The total number of active providers using its virtual care platform grew to around 102,000 during the quarter, up 25% compared to 81,000 a year ago. * * *
Amwell has been making significant investments in its new virtual care platform, Converge. Announced in April, Converge makes all of Amwell’s products and programs, plus third-party applications, available in one place. * * *
The company is in the process of migrating its customers over to the new platform. About 10% of the company’s virtual visits occurred through Converge in the first quarter, up 40% compared to the fourth quarter, said Ido Schoenberg, chief executive officer. The first wave of upgrades will focus on hospital systems and then move to health plans, executives said.
“The market increasingly appreciates that automation is a compelling new element of digital healthcare and they require a trusted partner to provide integrated automation into their care delivery workflows,” he told analysts during the company’s first-quarter earnings call Monday.
Healthcare Dive meanwhile looks back at large health insurers’ reports on first-quarter 2022 earnings.
FedWeek compares annuitant eligibility rules for FEHB vs. FEDVIP and concludes that FEDVIP has more flexible rules. Why not?, considering that FEHB provides a government contribution while FEDVIP is enrollee pay-all. It’s still worth knowing the differences.
COVID-19 vaccinations prevented an estimated 107,000 Medicare hospitalizations between January and May 2021, resulting in $2.6 billion in savings for Medicare and Medicare Advantage plans, according to a new report by the Department of Health and Human Services. The report estimates the impact of COVID-19 vaccination during a five-month period shortly after the first vaccine was authorized and recommended for health care workers and elderly people in long-term care facilities. Future analyses will examine hospitalizations prevented by vaccination during the delta and omicron waves, HHS said.
“Paxlovid does what it has to do: it reduces the viral load,” Chief Executive Officer Albert Bourla said in an interview. “Then your body is supposed to do the job.” But for unknown reasons, the CEO said, some patients aren’t able to clear the virus with the first course of treatment.
In cases where virus levels do rebound, Bourla said, “then you give a second course, like you do with antibiotics, and that’s it.”
As noted in the article, the fly in the ointment is that the FDA emergency use authorization does not expressly approve a second course of the medication.
From the Rx coverage front
MedCity News reports on Bristol Myers Squibb’s (BMS) NEX-T program to improve CAR-T treatments.
The company has described NEX-T as changes to manufacturing driven by the translational insights it has gleaned from treating thousands of patients with its CAR T therapies. In addition to a faster turnaround time, the strategy is intended to reduce the costs of the overall process.
One of the key goals for the next-generation of cell therapies is treating solid tumors.
Another strategy that BMS is pursuing is going after two targets with a single therapy, reducing the risk that a tumor escapes from the treatment
Looking at the flip side of this coin, Forbes reports
Health plans and pharmacy benefit managers (PBMs) that manage drug costs speaking at this year’s Asembia Specialty Pharmacy Summit in Las Vegas say specialty drugs now account for 50% or greater of the total prescription spending they manage. In some cases, employer clients are seeing specialty costs account for 60% or even greater of their total drug spending.
“It really is frightening for our clients,” Lucille Accetta, senior vice president of pharmacy benefit management and specialty product development at CVS Health told hundreds of attendees at the Asembia event, which runs through Thursday and drew more than 5,000 people from the healthcare industry. “We have to be the best purchaser for our clients.” * * *
To reign in the costs of prescription drugs while maintaining access to life-saving treatments, health plans and pharmacies say they are more closely monitoring patients as soon as they are on the drug, said Rina Shah, group vice president of pharmacy operations and services at Walgreens.
The Forbes article adds
Abarca Health [is] an independent PBM that manages more than $5 billion in drug costs annually for more than four million Americans has executives at this week’s Asembia meeting talking up its efforts to better manage specialty pharmacy costs.
The company’s Assura solution launched earlier this year “guarantees the net cost of drugs, including specialty medications, by offering an annual fixed per script cost for a health plan’s entire population,” Abarca said in announcing the new pricing solution earlier this year. The guarantee, Abarca CEO Jason Borschow says, is adjusted each year based on drug benefit coverage changes.
Even as COVID-19’s benefit waned, new plan members across multiple product lines helped drive CVS to $2.3 billion in profit in the first quarter, slightly higher than the $2.2 billion brought in at the same time last year.
In results published Wednesday, the company beat Wall Street expectations on earnings and revenue, with a topline of $76.8 billion, up 11% year over year.
Fierce Healthcare explains how CVS has shifted from a retail to a digital marketing focus.
Moderna Inc. MRNA 5.81% said that its first-quarter revenue and profit tripled from a year earlier on higher sales of its Covid-19 vaccine and that a fall booster-shot campaign could drive continued sales gains.
The biotechnology company’s revenue topped $6 billion in the period ended March 31, beating analyst expectations and rising from $1.94 billion a year earlier, driven almost entirely by sales of its messenger RN
Moderna Inc. MRNA 5.81% said that its first-quarter revenue and profit tripled from a year earlier on higher sales of its Covid-19 vaccine and that a fall booster-shot campaign could drive continued sales gains.
The biotechnology company’s revenue topped $6 billion in the period ended March 31, beating analyst expectations and rising from $1.94 billion a year earlier, driven almost entirely by sales of its messenger RNA-based vaccine, branded as Spikevax. * * *
From the health risks front, MedPage Today explains that
Seven risk factors, some modifiable and some not, accounted for the vast majority of risk for first-time acute myocardial infarction (MI) in young adults, according to a case-control study.
The seven factors — diabetes, depression, hypertension, smoking, family history of premature MI, low household income, and hypercholesterolemia — were responsible for 83.9% of the total acute MI risk in young women and 85.1% of the risk in young men, reported Harlan Krumholz, MD, SM, of Yale New Haven Hospital in New Haven, Connecticut, and colleagues.
Older adults who obtain a flu shot are less likely to suffer a heart attack or stroke and are at lower risk for death from heart-related health events in the year after getting vaccinated, an analysis published Friday found.
Just under 4% of older adults vaccinated against the seasonal virus experienced a “cardiovascular event” within the next year compared to just over 5% of those who did not receive the shot, data published Friday by JAMA Network Open showed.
From the meetings department,
HHS provides a readout of a high-level meeting among Labor Department, health insurance and business executives “to discuss compliance with the Mental Health Parity and Addiction Equity Act, adequacy of in-network providers and mental health and substance use disorder treatment during the pandemic, as the nation observes Mental Health Awareness Month.”
The National Committee for Quality Assurance reviews the presentations at last week’s Quality Talks conference.
From the federal employee benefits front, FedWeek discusses OPM’s planned improvement to processing retirement applications as unveiled in the Fiscal Year 2023 budget document. Processing federal retirement benefits will be a heavy lift for OPM until Congress simplifies the pension calculation.
MedPage Today brings us up to date on the whereabouts of Omicron BA 2.12.1.
“What we’re seeing right now is a version of the virus that is much more transmissible than previous versions of the virus, perhaps, but also less likely to cause severe disease,” Perry Halkitis, PhD, MPH, dean of the Rutgers School of Public Health, told MedPage Today.
The FEHBlog heard a fascinating talk about the Long Covid or PASC on the second and final day of the 2022 OPM AHIP Carrier Conference. Dr. Micheal Brode explained that PASC usually is evidenced by fatigue, brain fog, or exertional fatigue more than 12 weeks after the first symptoms of Covid. People afflicted by PASC typically, but not always, were hospitalized when Covid was in its acute opening phase. Covid vaccinations reduce the risk of contracting PASC by at least 50%, but they don’t prevent PASC. Although it’s premature for evidenced-based treatment guidelines to exist, Dr. Brode complimented the work of the PASC Collaborative to get to that point expeditiously. Most PASC patients recover slowly with medical care, although some PASC patients have permanent disabilities. Dr. Brode reminded the audience that Covid is a multi-system disease, not only a lung disease. PASC’s recently added ICD-10 code is U09.9.
The American Hospital Association adds, “Moderna today asked the Food and Drug Administration to authorize for emergency use its COVID-19 vaccine in children aged six months through 5 years, citing previously released data estimating the vaccine’s efficacy against the omicron variant in this age group was similar to that in adults, with a favorable safety profile.”
Humana has released its 1st Quarter 2022 earnings. Fierce Healthcare provides background on the favorable report.
Fierce Healthcare informs us, “Walmart’s telehealth provider, MeMD, is rolling out the virtual diabetes program as a standalone service or as part of a comprehensive medical and behavioral telehealth program for enterprise customers and health plans. The retail giant collaborated with the American Diabetes Association on the virtual program, which was developed to help employees and members close gaps in diabetes management through early intervention, Walmart Health executives said.”
From the drug research front, BioPharma Dive tells us
Eli Lilly’s experimental diabetes shot tirzepatide helped obese people who have an underlying medical condition lose more than 15% of their body weight in a late-stage clinical trial. At the highest dose tested, patients receiving the weekly injection lost, on average, 21% of their body weight, Lilly said in a press release Thursday.
The data suggests tirzepatide could challenge similar drugs marketed by Danish drugmaker Novo Nordisk, which earned about $1.2 billion when prescribed for obesity in 2021. Novo’s weekly weight-loss shot Wegovy helped patients with medical complications lose an average of 15% of their body weight in clinical testing.
Wall Street analysts forecast swift growth for obesity drugs in coming years as patients, doctors and insurers acknowledge the effectiveness of newer agents like Wegovy and tirzepatide. Wegovy sales alone are expected to reach $5.5 billion in 2026, according to consensus estimates highlighted by Cantor Fitzgerald analyst Louise Chen in January.
Change is the biggest constant for the federal workforce after two years in a pandemic that capsized government operations. Despite the upheaval, employee engagement remained relatively steady over the last year, dropping just one point between 2020 and 2021, from 72% down to 71%.
But other factors, like employees’ job and pay satisfaction, declined in 2021 compared to 2020. The overall index points for global satisfaction dropped as well, from 69% down to 64%.
As part of his fiscal 2023 budget proposal, [President] Biden proposed an average pay increase of 4.6% for civilian federal workers and members of the military, which, if implemented, would mark the biggest raise the federal workforce has seen in 20 years. Although it is unclear how that raise would be broken up between across-the-board increases to basic pay and an average boost to locality pay, traditionally, 0.5% of the pay raise has been set aside for locality pay increases.
In a letter, [62] House Democrats led by Rep. Gerry Connolly, D-Va., pressed the leadership of the House Appropriations Committee to go further than the president and endorse a 5.1% average pay increase for feds, reflecting legislation introduced by Connolly and Sen. Brian Schatz, D-Hawaii, that would grant federal employees a 4.1% across-the-board boost to basic pay and a 1.0% average increase in locality pay.
And don’t forget that this Saturday, April 30, is National Prescription Drug Take-Back Day.
From the Capitol Hill front, Congress is on a State / District work period for the next two weeks.
Medpage Today identifies the likely winners and losers if the Senate joins the House of Representatives in capping insulin cost-sharing at $35 per dose. There are no surprises.
From the federal employment front, Govexec tells us
The U.S. Postal Service has converted 63,000 part-time or non-permanent workers into career positions, with leadership saying it has helped stabilize the workforce after years of escalating turnover. * * *
The Postal Service ended 2021 with nearly 517,000 career employees, its highest total since 2012. The non-career workforce has remained fairly steady in recent years at 136,000.
This factoid is worth noting because career employees typically are eligible for FEHB coverage while part-timers and non-permanent workers are not.
From the Omicron and siblings front, the Wall Street Journal informs us about the BA.2-related numbers to watch when considering whether or not to take additional Covid precautions. For example,
Hospitalization rates are likely a more accurate indicator of transmission and reflect the severity of infections, some scientists say. A related useful metric: the number of people visiting emergency rooms with influenza-like illnesses, which the CDC tracks and publishes nationally; New York has data, too. Scientists say BA.2 is more transmissible than the original Omicron variant but not more dangerous. * * *
UNC’s Dr. Lessler says the [CDC’s Communities] map is useful for those who aren’t at high risk for severe Covid and don’t have close contact with those who are. “It can serve as a good lower limit for how cautious to be,” he says.
The CDC’s surveillance of wastewater for Covid-19 is also telling, he says, though it is based on limited samples. Some wastewater data show readings from the Northeast, in particular, have been edging higher from low levels. * * *
Should you decide that the level of Covid-19 circulating is too high for your comfort, Dr. Varma advises putting a few measures in place:
— Make sure you’re up to date with Covid vaccinations and boosters for which you’re eligible.
— Ensure that you have a supply of rapid antigen tests; one pack per family member is a good rule of thumb.
— Improve indoor ventilation when you have visitors over or if someone in your household gets Covid-19.
— Have the number of your local or state health department on hand so you can get antiviral pills if you qualify and fall sick.
And, if you test positive, follow the latest guidelines recommended by the CDC and your doctor.
From the opioid epidemic front
NPR discusses draft CDC guidance on prescribing opioids that will replace the current guidance that was issued in 2016.
MedPage Today suggests that doctors should not prescribe opioids without first preparing a deprescribing plan for the patient.
A deprescribing plan involves laying out a specific path for reducing, and then eliminating, opioid use even before the first prescription is written. It is often a way for physicians to involve other resources, including mental health care, community support, and social services to assist the patient as opioid dosage gradually falls.
Importantly, the plan should not be an act of enforcement, but rather, the product of physician and patient working together. Properly structured, the plan will give the patient confidence that an opioid prescription may help relieve pain in the short run but will not lead to dependence or addiction in the long term. The goal is to produce a better outcome for the patient than is possible with continued opioid use.
From the telehealth front, mHealth Intelligence reports
MemorialCare in Fountain Valley, California, is partnering with TytoCare to enhance its telehealth services.
TytoCare provides virtual home examination and diagnosis solutions, including a hand-held tool for remotely examining the heart, lungs, skin, ears, throat, abdomen, and body temperature, and a telehealth platform for sharing exam data, conducting live video exams, and scheduling visits.
Through the new partnership, MemorialCare will expand its virtual care offerings. TytoCare’s handheld device will allow patients to perform guided medical exams with MemorialCare providers remotely. The device has received Food and Drug Administration approval.
Patients can use the TytoCare app to participate in video visits offered through MemorialCare’s Virtual Urgent Care service. Data from the remote exam is sent to MemorialCare providers through an encrypted network.
Providers can leverage exam data to diagnose and treat conditions and write a prescription if needed. The virtual visit is also downloaded into MemorialCare’s MyChart EMR system.
From the medical research department, STAT News reports
While CAR T-therapy has cured some people with blood cancers, this form of immunotherapy has so far produced lackluster results for solid tumors like lung or kidney cancer. But a new early-phase clinical trial presented on Sunday at the American Association of Cancer Research (AACR) conference suggests that CAR T-cells may be able to shrink some solid tumors — as long as it gets a boost from an mRNA vaccine from BioNTech.
The mRNA vaccine manufacturers worked on cancer cures before they pivoted to Covid in early 2020. It’s hopeful to see that BioNTech is back in cancer research.
The week is still young. But prospects for getting a bipartisan supplemental aid package for pandemic response efforts to President Joe Biden’s desk before a two-week recess seem increasingly remote.
Without a deal on amendments Republicans want to offer, the Senate on Tuesday rejected a procedural motion needed to begin debate on the bill, which would provide $10 billion for the Department of Health and Human Services to buy more therapeutics, vaccines and testing supplies and prepare for future virus variants.
Utah Sen. Mitt Romney, the lead GOP negotiator, said the underlying bill will have enough bipartisan support to pass if leaders can agree on an amendment process, but it’s an open question whether it will get done before the recess.
From the Omicron and siblings front, the Wall Street Journal reports
The Omicron BA.2 variant is increasing its share of U.S. cases and putting particular pressure on parts of the Northeast, where wastewater readings and Covid-19 cases have ticked upward again from low levels.
Recorded Covid-19 cases remain low nationally and hospitals are treating the smallest number of Covid-19 patients after any surge. Places where cases are rising, including New York, are reporting relatively small increases from recent troughs. The mixed signals are prompting officials to warn that BA.2 will likely lead to more viral transmission, but also hope among public-health experts that warming weather and built-up immunity in the population are muting the variant’s impact.
“There are certainly some big factors that are in our favor right now compared to the situation back in November and December,” said Bruce Y. Lee, professor of health policy and management at the City University of New York School of Public Health.
From the White House, the Administration announced
A “whole of government” effort to prevent, detect, and treat long Covid. Long Covid is a topic at the OPM AHIP FEHB carrier conference to be held virtually on April 27 and 28, 2022.
A regulatory fix to the so-called family glitch in the Affordable Care Act. The family glitch that this fix addresses stems from the fact that the ACA does not require employers to make contributions to family member coverage. “Should today’s proposed rule be finalized, family members of workers who are offered affordable self-only coverage but unaffordable family coverage may qualify for premium tax credits to buy ACA coverage.” In the FEHBlog’s personal experience, the unaddressed family glitch is that that small employers (generally under 50 employees) must pay for each family member’s coverage on an age rated basis instead of the plus one or plus and family rates that large employers are permitted to use. Pre-ACA, all employers could use the bucket approach to family member rating. The proposed regulation won’t fix that problem.
agencies (as described in section 3502(1) of title 44, United States Code, except for the agencies described in section 3502(5) of title 44, United States Code) with responsibilities related to Americans’ access to health coverage shall review agency actions to identify ways to continue to expand the availability of affordable health coverage, to improve the quality of coverage, to strengthen benefits, and to help more Americans enroll in quality health coverage. As part of this review, the heads of such agencies shall examine the following:
(a) policies or practices that make it easier for all consumers to enroll in and retain coverage, understand their coverage options, and select appropriate coverage;
(b) policies or practices that strengthen benefits and improve access to healthcare providers;
(c) policies or practices that improve the comprehensiveness of coverage and protect consumers from low-quality coverage;
(d) policies or practices that expand eligibility and lower costs for coverage in the ACA Marketplaces, Medicaid, Medicare, and other programs;
(e) policies or practices that help improve linkages between the healthcare system and other stakeholders to address health-related needs; and
(f) policies or practices that help reduce the burden of medical debt on households.
These are interesting objectives, but FEHB typically is not considered to be a employee benefit program and not a government health program.
From the healthcare business front
Beckers Hospital Review tells us “Walmart Health will open five new clinics in Florida, according to an April 5 press release.” Healthcare Dive offers a deep dive into Walmart’s healthcare efforts in the Sunshine State.
UnitedHealth Group’s Optum and Change Healthcare have further extended their merger agreement to Dec. 31. The extension comes ahead of a two-week trial to determine the deal’s fate.
The Department of Justice sued to block the merger in late February, alleging that the combination could allow UnitedHealth to get a leg up on its competitors in the insurance space. The deal was first announced in January 2021 and is valued at $8 billion in cash and $5 billion in debt.
The trial is set to begin on Aug. 1.
“The extended agreement reflects our firm belief in the potential of our combination to improve healthcare and in our commitment to contesting the meritless legal challenge to this merger,” the companies said in a joint statement Tuesday.
From the tidbits department
Shatterproof offers alcohol awareness resources in recognition of April being Alcohol Awareness Month.
Per Health Day, “Significantly higher average body mass index (BMI) and obesity prevalence rates were seen among U.S. adults during the COVID-19 pandemic, according to a study published online April 4 in the American Journal of Preventive Medicine.” The complete journal article is available here.
The same preventive medicine journal also offers an article on mortality rates of childbearing aged women in our country. “Given the high correlation between pregnancy-related mortality and all-cause mortality at the state level, addressing the structural factors that shape mortality risks may have the greatest likelihood of improving women’s health outcomes across the life course.”
The HHS Inspector General has created a website on telehealth.
The Office of Personnel Management last week offered guidance to agencies on how they should implement the recently enacted benefit providing federal workers with up to two weeks of paid bereavement leave following the death of a child.
The new leave was adopted as part of the 2022 National Defense Authorization Act, signed by President Biden last December.
In a memo to agency heads, OPM Director Kiran Ahuja wrote that although each agency is responsible for its own implementation of the new benefit, her agency wants to ensure that it is provided to employees across government “in an equitable and uniform way.”
Senate negotiators have reached agreement on a $10 billion pandemic relief package that includes funding for domestic needs but not international aid, according to two Senate aides who were not authorized to speak publicly.
The deal crystallizes an informal “agreement in principle” the parties reached last week to provide $10 billion for near-term pandemic needs by repurposing unspent funds from prior relief laws.
The White House backed the deal and urged Congress to pass the bill promptly, while noting it was less than the $22.5 billion the administration had requested for vaccines, boosters, treatments and testing.
“We will continue to work with Congress to fund our remaining domestic needs,” said Press Secretary Jen Psaki in a statement. She added that the White House would continue to press for funding global vaccination efforts.
The FEHBlog noticed that the Senate Homeland Security and Governmental Affairs Committee held a business meeting last Wednesday. The Committee favorably reported the President’s nomination of Kristin Boyd to be OPM Inspector General by voice vote (with Sen. Hawley (R Mo.) voting no). The next step for Ms. Boyd’s nomination is the Senate floor.
Last week, the House of Representatives passed a Secure 2.0 bill applicable to private sector defined contribution plans. The Senate is likely to approve the bill too. The Society for Human Resource Management has reviewed the bill’s provisions.
From the Omicron and siblings front —
Becker’s Hospital Review informs us “The World Health Organization is monitoring a new omicron variant — dubbed XE — that’s a hybrid of BA.1, the original omicron strain, and BA.2, a highly transmissible subvariant.” The hybrid is estimated to be 10% more contagious that BA.2.
American Hospital Association tells us “Beginning today through the end of the public health emergency, Medicare Part B beneficiaries may obtain up to eight free over-the-counter COVID-19 tests per month through eligible health care providers and pharmacies, the Centers for Medicare & Medicaid Services announced.” Medicare Part B beneficiaries can obtain the free tests by showing their Medicare identification card.
The American Medical Association discusses “How we will know when COVID-19 has become endemic.” The FEHBlog tends to think that we are there.
The Centers for Disease Control announced
The new nationwide Test to Treat initiative provides quick access to free treatment for COVID-19. Through this program, people can get tested and – if they are positive and treatments are appropriate for them – receive a prescription from a health care provider, and have their prescription filled all at one location. These “One-Stop Test to Treat” sites are available at hundreds of locations nationwide, including pharmacy-based clinics, federally qualified health centers, and long-term care facilities. People can continue to be tested and treated by their own health care providers who can appropriately prescribe these oral antivirals at locations where the medicines are distributed. A call center 1-800-232-0233 is available every day from 8:00 am to midnight ET to get help in more than 150 other languages. The Disability Information and Access Line is available to help people with disabilities access services. Call 1-888-677-1199, Monday-Friday from 9:00 am to 8:00 pm ET or email DIAL@usaginganddisability.org.
From the CMS front, the agency announced that “the updated MMSEA Section 111 GHP User Guide version 6.5 has been posted to the GHP User Guide page on CMS.gov. Refer to Chapter 1 for a summary of updates.” Section 111 is a system that has been in place for about 12 years. Section 111 helps CMS keep tabs on Medicare beneficiaries and beneficiaries using data group health plans, including FEHB plans, automobile and liability insurers, and attorneys for injured Medicare beneficiaries.
CMS also released “the Announcement of Calendar Year (CY) 2023 Medicare Advantage (MA) Capitation Rates and Part C and Part D Payment Policies (the Rate Announcement).”
From the federal employment front, Govexec reports
Federal employees can hold elected partisan office while also working at their agencies, a key panel found in a ruling setting a new precedent for civil servants.
Rodney Cowan did not have to give up his role as a county commissioner in Tennessee or be removed from his job with the U.S. Postal Service, the recently reconstituted central body of the Merit Systems Protection Board said in a decision last week. It was one of the first decisions of MSPB’s central board as it addresses its backlog of more than 3,500 cases that have piled up during its five years without a quorum.
The FEHBlog doubts that we have heard the last word on this issue.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.