Last night, the FDA granted Moderna emergency use authorization for administering its mRNA based COVID-19 vaccine to Americans aged 18 and older. About an hour ago, the CDC’s Advisory Committee seconded this decision which means that health plans, including FEHB plans, must begin to provide in-network and out-of-network coverage for administration of the Moderna vaccine on January 3, 2021. That is certainly good news.
Last night, as CBS News reports, the Senate joined the House of Representatives in approving a two day extension of the continuing resolution funding the federal government, and the President signed the resolution into law. The Hill adds this afternoon that
Speaker Nancy Pelosi (D-Calif.) told Democratic House members during a conference call Saturday that a deal is within reach as soon as negotiators hammer out an agreement on language being pushed by Sen. Pat Toomey(R-Pa.) to wind down the Federal Reserve credit lending facilities. Pelosi told colleagues that the “good news” is “we’re right within reach” of resolving that disagreement.
In other news —
The American Medical Association offers advice on which masks work best in warding off COVID-19.
The federal government’s Cybersecurity and Infrastructure Security Agency (“CISA”) offered updated guidance today on the SolarWinds backdoor hack.
Bloomberg provided this interesting observation on the scope of this hack:
At least 200 organizations, including government agencies and companies around the world, have been hacked as part of a suspected Russian cyber-attack that implanted malicious code in a widely used software program, said a cybersecurity firm and three people familiar with ongoing investigations.
The number of actual hacking victims has been one of many unanswered questions surrounding the cyber-attack, which used a backdoor in SolarWinds Corp.’s Orion network management software as a staging ground for further attacks.
As many as 18,000 SolarWinds’ customers received a malicious update that included the backdoor, but the number that was actually hacked — meaning the attackers used the backdoor to infiltrate computer networks — is likely to be far fewer.
Based on the CDC’s Cases in the U.S. website, here is the FEHBlog’s chart of new weekly COVID-19 cases and deaths over the 20th through 50th weeks of this year (beginning May 14 and ending December 16; using Thursday as the first day of the week in order to facilitate this weekly update):
and here is the CDC’s latest overall weekly hospitalization rate chart for COVID-19:
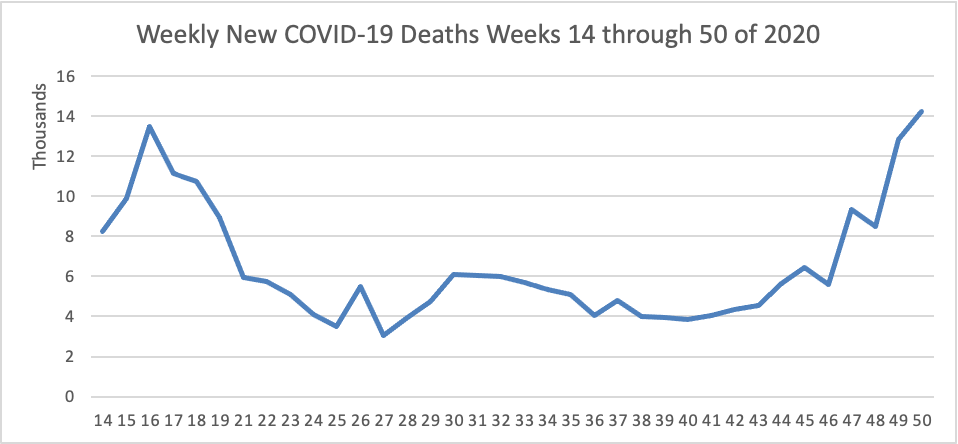
The FEHBlog has noted that the new cases and deaths chart shows a flat line for new weekly deaths because new cases greatly exceed new deaths. Accordingly here is a chart of new COVID-19 deaths over the period (April 2 through December 9). The FEHBlog extended this chart from April 2 to May 14 in order to display the previous high for this sad metric.
The CDC’s current Fluview report continues to state “Seasonal influenza activity in the United States remains lower than usual for this time of year.” So Americans must be doing something right.
1) substantial increases in drug overdose deaths across the United States, primarily driven by rapid increases in overdose deaths involving synthetic opioids excluding methadone (hereafter referred to as synthetic opioids), likely illicitly manufactured fentanyl; (2) a concerning acceleration of the increase in drug overdose deaths, with the largest increase recorded from March 2020 to May 2020,coinciding with the implementation of widespread mitigation measures for the COVID-19 pandemic; (3) the changing geographic distribution of overdose deaths involving synthetic opioids, with the largest percentage increases occurring in states in the western United States; (4) significant increases in overdose deaths involving psychostimulants with abuse potential (hereafter referred to as psychostimulants) such as methamphetamine; and
The House [of Representatives] passed a two-day spending bill Friday evening, sending it over to the Senate in a bid to prevent a partial government shutdown after midnight, as congressional leaders struggled to wrap up negotiations on a coronavirus relief package.
In the Covid-19 talks, negotiators were still wrestling Friday to close differences on the Federal Reserve’s emergency lending powers among other final snags. Leaders have aimed to pair the passage of the Covid-19 aid bill with a broader spending bill.
The FEHBlog expected a little bit longer extension but a two day extension suggests that the compromise on the COVID-19 relief bill is near. The FEHBlog cannot believe that with the Georgia Senate primary approaching on January 5 that either party would risk a government shutdown or not COVID-19 relief. But we shall see.
In that regard, the FEHBlog read on the American Hospital Association’s daily report about this health system letter to Congress, delivered today, suggesting that there is some crazy language in that bipartisan surprise billing proposal. Again, we shall see.
HHS’s Office for Civil Rights issued “guidance on how the Health Insurance Portability and Accountability Act of 1996 (HIPAA) permits covered entities and their business associates to use health information exchanges to disclose protected health information (PHI) for the public health activities of a public health authority. The guidance provides examples relevant to the COVID-19 public health emergency on how HIPAA permits covered entities and their business associates to disclose PHI to an HIE for reporting to a PHA that is engaged in public health activities.”
The FEHBlog just watched the Food and Drug Administration’s (“FDA”) Vaccines and Biological Products Advisory Committee unanimously recommend by a 20-0 vote (one abstention) that the FDA grant emergency use authorization (EUA) to the Moderna COVID-19 vaccine. Last week the same Committee appro/ved the Pfizer-BioNTech vaccine by a 17-4-1 vote. Both vaccines rely on mRNA technology. In the FEHBlog’s view, the difference between the votes is that Moderna limited its EUA application to people aged 18 or older while Pfizer’s extension of the EUA to sixteen and seventeen year old people was controversial. If recent history is any guide, the FDA can be expected to grant the EUA tomorrow and over the weekend the CDC’s Advisory Committee on Immunization Practices will trigger health plan coverage of the vaccine effective fifteen days later.
Politico reports that the Johnson & Johnson vaccine will be presented to this FDA committee in late January 2021. “The vaccine is the only one among the frontrunners that is given as a single dose. “Because it’s a one dose vaccine, they can really scale up very quickly,” said Moncef Slaoui, the chief adviser to Operation Warp Speed.
Becker’s Health IT reports that “Healthcare workers in Indiana who tried signing up for the first round of COVID-19 vaccinations Dec. 14 overwhelmed the state’s enrollment website, resulting in down time, according to Indianapolis NBC affiliate WTHR.” Why is this good news? Because now that the COVID-19 vaccine is a reality, people will want the jab as the call it in Britain. That’s human nature.
The Wall Street Journal reports that “The Food and Drug Administration [“FDA’] said Tuesday that the Covid-19 vaccine developed by Moderna Inc. was “highly effective,” setting the stage for an emergency authorization later this week that would add a second vaccine to the arsenal against the pandemic.” Here’s a link to the Moderna briefing document for Thursday’s meeting with the FDA’s Vaccines and Related Biological Products Advisory Committee.
A friend of the FEHBlog pointed out the following encouraging FDA announcement
Today, the U.S. Food and Drug Administration issued an emergency use authorization (EUA) for the first over-the-counter (OTC) fully at-home diagnostic test for COVID-19. The Ellume COVID-19 Home Test is a rapid, lateral flow antigen test, a type of test that runs a liquid sample along a surface with reactive molecules. The test detects fragments of proteins of the SARS-CoV-2 virus from a nasal swab sample from any individual 2 years of age or older.
“Today’s authorization is a major milestone in diagnostic testing for COVID-19. By authorizing a test for over- the-counter use, the FDA allows it to be sold in places like drug stores, where a patient can buy it, swab their nose, run the test and find out their results in as little as 20 minutes,” said FDA Commissioner Stephen M. Hahn, M.D. “As we continue to authorize additional tests for home use, we are helping expand Americans’ access to testing, reducing the burden on laboratories and test supplies, and giving Americans more testing options from the comfort and safety of their own homes.”
The announcement today of the first fully at-home OTC COVID-19 diagnostic test follows last month’s authorization of the first prescription COVID-19 test for home use and last week’s announcement of the first non-prescription test system, in which a lab processes the self-collected sample. The FDA has authorized more than 225 diagnostic tests for COVID-19 since the start of the pandemic, including more than 25 tests that allow for home collection of samples, which are then sent to a lab for testing. The Ellume COVID-19 Home Test is the first COVID-19 test that can be used completely at home without a prescription.
On the omnibus / COVID-19 relief bill front, the Wall Street Journal reports
The top four congressional leaders discussed a coronavirus relief package and sweeping spending bill on Tuesday and planned to return for another meeting in the evening, as lawmakers raced to reach an agreement before critical support programs expire at year’s end.
House Speaker Nancy Pelosi (D., Calif.), Senate Majority Leader Mitch McConnell (R., Ky.), Senate Minority Leader Chuck Schumer (D., N.Y.) and House Minority Leader Kevin McCarthy (R., Calif.) first conferred in the afternoon, with the meeting of both parties’ leaders a signal that they could be ready to make the difficult decisions needed to cut a deal.
The group will meet again late Tuesday.
“We’re continuing to work. I think there’s progress. We’ll get back together,” Mr. McCarthy said following the afternoon meeting.
Treasury Secretary Steven Mnuchin, who spoke to Mrs. Pelosi earlier Tuesday for more than an hour, also joined the first meeting by phone.
The legislative text must be released tomorrow if Congress want to stick with the current December 18 deadline for action.
A friend of the FEHBlog pointed out the Office of Management and Budget’s Office of Information and Regulatory Affairs has issued its Fall 2020 Unified Agenda of “Regulatory and Deregulatory Actions. Here’s a link to the OPM agenda. The FEHBlog noticed a FEHBP centralized enrollment proposed rule and a final FEHBAR rule involving the Truth in Negotiations Act threshold change which the FEHBlog called to OPM’s attention.
In other healthcare news
Health Payer Intelligence offers “Five Pivotal Payer Industry Trends To Watch in 2021.”
Healthcare Finance News reports that various healthcare trade associations have asked a federal district court in Maryland to preliminarily enjoin implementation of the Trump Administration’s Medicare Part B international drug price index pilot scheduled for January 1, 2021. The motion was filed on December 10 and the government filed its opposition today.
A friend of the FEHBlog pointed out this NIH press release on the state of bad teenager habits.
Findings released today from the most recent Monitoring the Future (MTF) survey of substance use behaviors and related attitudes among teens in the United States indicate that levels of nicotine and marijuana vaping did not increase from 2019 to early 2020, although they remain high. The annual MTF survey is conducted by the University of Michigan’s Institute for Social Research, Ann Arbor, and is funded by the National Institute on Drug Abuse (NIDA), part of the National Institutes of Health.
In the four years since the survey began including questions on nicotine and marijuana vaping, use of these substances among teens have increased to markedly high levels From 2017 to 2019, the percentage of teenagers who said they vaped nicotine in the past 12 months roughly doubled for eighth graders from 7.5% to 16.5%, for 10th graders from 15.8% to 30.7%, and for 12th graders from 18.8% to 35.3%. In 2020, the rates held steady at a respective 16.6%, 30.7%, and 34.5%. However, somewhat encouragingly, daily, or near daily (20 occasions in the past 30 days), nicotine vaping declined among 10th and 12th graders from 2019 to 2020, by close to half — from 6.8% to 3.6% in 10th grade and from 11.6% to 5.3% in 12th grade.
STAT News offers a portrait of the COVID-19 virus at one year — what scientists know about how it spreads, infects, and sickens. Meanwhile, the AP provides its perspective on today’s first COVID-19 vaccinations, which should be view as a miracle as vaccines normally take at least four years to develop.
Healthcare Dive and Revcycle Intelligence discuss industry reaction to the bipartisan, bicameral surprise billing legislation introduced in Congress last week. The articles make it clear that neither providers nor payers are entirely happy with the legislation and that the legislators’ goal is to attach the bill to this week’s must pass omnibus spending bill (“the omnibus”). It could go.
A friend of the FEHBlog pointed out today another bill that could get attached to the omnibus. Last week the House passed H.R. 7898 which would permit HHS’s Office for Civil Rights to mitigate HIPAA fines and other remedies when the covered entity or business associate has adequately demonstrated that it “had, for not less than the previous 12 months, recognized security practices in place.” “The term ‘recognized security practices’ means the standards, guidelines, best practices, methodologies, procedures, and processes developed under section 2(c)(15) of the National Institute of Standards and Technology Act, the approaches promulgated under section 405(d) of the Cybersecurity Act of 2015, and other programs and processes that address cybersecurity and that are developed, recognized, or promulgated through regulations under other statutory authorities. Such practices shall be determined by the covered entity or business associate, consistent with the HIPAA Security rule (part 160 of title 45 Code of Federal Regulations and subparts A and C of part 164 of such title).” That’s quite reasonable and equitable.
Bloomberg reports today that legislative work on the omnibus itself remains on track. Also the FEHBlog appreciated Bloomberg’s insights into the COVID-19 relief bill which would be the key measure to be attached to the omnibus. What better time than now for Christmas tree legislation” In any event, according to Bloomberg,
[U.S Senator John] Cornyn [R TX] said the $908 billion bipartisan proposal unveiled Monday isn’t likely to go forward by itself but will be used as jumping-off point for the leaders from both parties in both chambers. ”It’s having a positive influence on what will ultimately included,” Cornyn said of the bipartisan proposal.
Forbes provides more background on the status of the COVID-19 relief legislation for those who are interested (as the FEHBlog is).
While the FEHBlog is a subscriber to the WSJ, Bloomberg and STAT News, among others, he does not subscribe to Modern Healthcare. That’s difficult at this time of year because he does get a kick out of their list of the 100 people who have most influence on U.S. healthcare. Fortunately, AHIP provided a list of their members’ executives who made the list. Congratulations to them.
Last night, the Food and Drug Administration announced that it has granted emergency use authorization for administering the Pfizer-BioNTech COVID-19 vaccine to people aged 16 and older in our country.
Initial supplies will be limited. Pfizer projects it will deliver 25 million doses to the U.S. this year, including 2.9 million doses the first week. Inoculation requires two doses three weeks apart, so only half that many people will be vaccinated. States will decide where many doses go.
Gen. Gustave Perna, chief operating officer of the federal government’s Operation Warp Speed vaccine effort, said Saturday the initial supplies will be distributed among 636 locations nationwide, with 145 sites expected to get the doses Monday.
Another 425 sites should receive deliveries Tuesday, while the remaining 66 sites are slated to get their supplies Wednesday, Gen. Perna said.
The U.S. government is dividing up the supply among states, territories and jurisdictions based on their adult populations.
First in line will largely be the nation’s 21 million health-care workers such as doctors and nurses treating Covid-19 patients, as well as residents of nursing homes and other long-term care facilities.
The Centers for Disease Control’s Advisory Committee for Immunization Practices (“ACIP”) made this phase 1A distribution recommendation earlier this month. Medscape reports that at a meeting held today,
ACIP voted 11-0, with three recusals, to recommend use of the Pfizer-BioNTech mRNA vaccine in individuals 16 years or older according to the guidelines of the Food and Drug Administration’s (FDA’s) emergency use authorization issued on Friday.
The panel also voted unanimously to include the vaccine in 2021 immunization schedules. All panel members said the recommendation should go hand-in-hand with ACIP’s previous recommendation on December 1 that allocation of the vaccine be phased-in, with health care workers and residents and staff of long-term care facilities in phase 1a, as reported byMedscape Medical News.
Of course, more medical guidance will be forthcoming as the vaccine is rolled out to the general public. To that end,
Peter Marks, MD, PhD, director of the FDA’s Center for Biologic Evaluation and Research (CBER) clarified this in a briefing on December 12, noting that women who are pregnant or lactating can make the decision in consultation with their physician. And, he said, patients with any other history of allergy should be able to safely get the vaccine.
The bottom line is that
Committee members breathed a sigh of relief at the end of the 2-day meeting, saying that although the Pfizer vaccine is not perfect, it represents a scientific milestone and a significant advance against the continuing march of the SARS-CoV-2 pandemic.
“This vaccine and future vaccines do provide a promise for a lot of progress in the future,” said panelist Beth P. Bell, MD, MPH, clinical professor of global health at the University of Washington School of Public Health in Seattle.
Peter Szilagyi, MD, MPH, executive vice-chair and vice-chair for research at the University of California, Los Angeles pediatrics department, said, “I’m really hopeful that this is the beginning of the end of the coronavirus pandemic.”
Thank goodness.
Pursuant to the CARES Act, health plans, including FEHB plans, become obligated to cover administration of this vaccine to its members with no cost sharing fifteen days from now, December 27, 2020.
Based on the CDC’s COVID Data Trackers website, here is the FEHBlog’s chart of new weekly COVID-19 cases and deaths over the 20th through 49th weeks of this year (beginning May 14 and ending December 9; using Thursday as the first day of the week in order to facilitate this weekly update):
and here is the CDC’s latest overall weekly hospitalization rate chart for COVID-19:
It’s interesting that the weekly rate dropped two weeks in a row. Typically the chart would show a one week drop which the FEHBlog discounted.
The FEHBlog has noted that the new cases and deaths chart shows a flat line for new weekly deaths because new cases greatly exceed new deaths. Accordingly here is a chart of new COVID-19 deaths over the same period (May 14 through December 9):
The FEHBlog’s record high for weekly deaths remains 13,504 for the week ended April 22 which we now are approaching.
On the brighter side, the Wall Street Journal reports that
The U.S. Food and Drug Administration said it was finalizing the work needed to clear a Covid-19 vaccine developed byPfizer Inc. and German partner BioNTech SE, after the injection was endorsed by an expert panel. “We could see people getting vaccinated Monday, Tuesday of next week,” Health and Human Services Secretary Alex Azar said on ABC’s “Good Morning America.”
Fierce Healthcare reports that “CVS [Health] is planning to begin administering COVID-19 vaccines in nursing homes beginning on Dec. 21, a top executive told Reuters.”
Govexec.com reports that “Civilian federal personnel are likely to begin receiving COVID-19 vaccinations as soon as Monday, officials said on Friday, though only [healthcare] employees at certain offices will receive the doses directly from their agencies. Govexec.com offered the most details on the Defense Department’s plans which provide a helpful perspective
The Defense Department also anticipates vaccinating 44,000 employees next week, officials said on Wednesday, the vast majority of whom will be health care staff. The Pentagon plans to provide vaccines to both military and civilian staff, though it has not committed to vaccinating to its entire civil service workforce.
“The eligibility we defined in terms of dependents, select contractors, civilian employees, and it’s going to be then how do they match up in terms of the prioritization tiers,” said Tom McCaffery, the assistant secretary of Defense for Health Affairs.
In the initial phase, Defense will target health care workers who are closest to patients, early emergency responders and public security staff. Defense will distribute vaccines to 16 sites in that phase, 13 of which are located within the United States. McCaffery said the department recently held a “virtual tabletop exercise” to go through the first phase “in great detail to ensure seamless distribution and dissemination” of the vaccine. Defense will ultimately be responsible for vaccinating millions of individuals, including active duty personnel, civilian workers, at-risk dependents and some contractors.
All told, Defense maintains 83 sites that have ultra-cold storage, including all 13 of those in the initial distribution.
will purchase an additional 100 million doses of COVID-19 vaccine candidate, called mRNA-1273, from Moderna.
If authorized by the U.S. Food and Drug Administration for emergency use as outlined in agency guidance, doses of the vaccine will begin shipping immediately. The vaccine would be provided at no cost to Americans. Vaccine administration costs for private-sector administration partners will be covered by healthcare payers: private insurance, Medicare or Medicaid, and an HHS program to cover COVID-19 costs for the uninsured which is reimbursing the provider at Medicare rates from the provider relief fund.
Under the agreement, Moderna will leverage its U.S.-based manufacturing capacity to fill, finish and ship vials of mRNA-1273 as the bulk material is produced. The additional doses ordered today provide for continuous delivery through the end of June 2021. This strategy will help meet the anticipated demand for mRNA-1273 and safely accelerate the delivery schedule for all 200 million doses the U.S. government is purchasing.
“Securing another 100 million doses from Moderna by June 2021 further expands our supply of doses across the Operation Warp Speed portfolio of vaccines,” said HHS Secretary Alex Azar. “This new federal purchase can give Americans even greater confidence we will have enough supply to vaccinate all Americans who want it by the second quarter of 2021.”
In other news,
Congress approved the one week long extension of the continuing resolution funding the federal government. The new deadline is December 18 and Federal News Network reports that “Negotiators on a $1.4 trillion catchall spending bill appeared to be moving in a positive direction, said the chairman of the Senate Appropriations Committee, Sen. Richard Shelby, R-Ala.. This bill would serve as a vehicle to carry any year-end virus assistance.” Negotiations over that COVID-19 relief bill continue.
The HHS, the Labor Department, and the Treasury Department (a/k/a the tri-agencies) “announced a final rule that amends the [Affordable Care Act] requirements for grandfathered group health plans and grandfathered group health insurance coverage to preserve their grandfather status.”
The U.S. Supreme Court unanimously rejected an ERISA preemption challenge to an Arkansas state law regulating prescription benefit manager pricing of drugs. Here is Healthcare Dive’s report. This decision will raise healthcare prices in the FEHBlog’s opinion.
Govexec.com reports that President Trump is giving a half day off to federal employees on Christmas Eve.
The FEHBlog’s link to the HHS fact sheet on the proposed HIPAA Privacy Rule changes (posted yesterday) was inoperable until the FEHBlog fixed it tonight. Here’s a link. Have a good weekend.
A panel of outside experts on Thursday recommended the Food and Drug Administration issue an emergency use authorization to the Covid-19 vaccine being developed by Pfizer and BioNTech, a vaccine that appeared to be highly efficacious in a Phase 3 clinical trial.
The 17-4 vote came after a long day in which members of the Vaccines and Related Biological Products Advisory Committee, or VRBPAC, discussed a wide range of issues related to the vaccine, including concerns about vaccinating people with severe allergies and 16- and 17-year-olds, as well as issues regarding vaccination during pregnancy or lactation.
Although the FDA does not have to follow the panel’s recommendation, it is widely expected to do so. The rollout of Covid-19 vaccine could then begin in the United States in a matter of days.
The FEHBlog watched on You Tube a good chunk of the discussion preceding the vote. The FEHBlog was surprised that the motion presented to the Committee would extend the emergency use authorization to 16 and 17 year olds. He thought that the the minimum age would be 18 years old, and the committee members who voted against the bill were pediatricians concerned about the 16 to 17 year olds. Another member who was not a physician argued that the emergency use authorization use authorization should be limited to health care workers and nursing home residents, the initial phases approved by the CDC’s Advisory Committee on Immunization Practices. In any event, the FEHBlog was pleased by the decisive vote. At the close of the virtual committee meeting the Chairman reminded the members that they would be meeting next Thursday December 17 to consider an emergency use authorization for the Modern vaccine.
Speaking of voting, the Senate did not take up today the one week long extension of continuing resolution funding the federal government or the FY 2021 national defense authorization act which the House approved yesterday. The Senate needs to act on the continuing resolution tomorrow. The Wall Street Journal reports that negotiations over another COVID-19 relief bill continue.
A friend of the FEHBlog called to his attention the Department of Health and Human Services website on combatting the COVID-19 virus. It’s quite comprehensive.
In other news today, the HHS Office for Civil Rights, which enforces the HIPAA Privacy and Security Rules, proposed changes to the Privacy Rule.
The proposed changes to the HIPAA Privacy Rule include strengthening individuals’ rights to access their own health information, including electronic information; improving information sharing for care coordination and case management for individuals; facilitating greater family and caregiver involvement in the care of individuals experiencing emergencies or health crises; enhancing flexibilities for disclosures in emergency or threatening circumstances, such as the Opioid and COVID-19 public health emergencies; and reducing administrative burdens on HIPAA covered health care providers and health plans, while continuing to protect individuals’ health information privacy interests.
A friend of the FEHBlog shared this HHS fact sheet on this proposed rule. The proposal has a 60 day comment deadline which will end during the Biden Administration.
HHS’s Centers for Medicare and Medicaid Services proposed new rules to crack down on prior authorization practice by Medicaid, CHIP, and QHP marketplace plans. (Medicare does not permit prior authorization.)
The rule would require payers in Medicaid, CHIP and QHP programs to build application programming interfaces (APIs) to support data exchange and prior authorization. APIs allow two systems, or a payer’s system and a third-party app, to communicate and share data electronically Payers would be required to implement and maintain these APIs using the Health Level 7 (HL7) Fast Healthcare Interoperability Resources (FHIR) standard.
Building on that foundational policy, this rule would require impacted payers to implement and maintain a FHIR-based API to exchange patient data as patients move from one payer to another. In this way, patients who would otherwise not have access to their historic health information would be able to bring their information with them when they move from one payer to another, and would not lose that information simply because they changed payers.
These proposed changes would also allow payers, providers and patients to have access to more information including pending and active prior authorization decisions, potentially allowing for fewer repeat prior authorizations, reducing burden and cost, and ensuring patients have better continuity of care.
The proposals are expected to take effect in January 2023. Good ideas. The pubic comment period ends on January 4, 2021, but the final rule no doubt will be in the hands of the Biden administration. The American Medical Association must be happy though.
In Govexec, benefits consultant Tammy Flanagan discusses FEHBP options for annuitants with primary Medicare A and B coverage. The FEHBlog is always impressed by the creative benefit designs that FEHB plan carriers offer members.
The House on Wednesday [December 9] passed a stopgap funding bill 343-67 that would give lawmakers an additional week to come up with full-year spending legislation and avoid a government shutdown later this month. The continuing resolution would last for one week, setting a new funding deadline of Dec. 18. The Senate must still pass the CR and President Trump must sign it by Friday to avoid a government shutdown, which both are expected to do.
The Wall Street Journal adds that “A flurry of competing proposals for another coronavirus relief package ricocheted around the Capitol Wednesday, as lawmakers hunted for ways to resolve a thorny debate over liability protections that has stymied progress for weeks.” A December 9 fact sheet on the bipartisan proposal was made available today. Check it out.
In Presidential transition news, President-elect Biden announced the following additional healthcare appointments earlier this week:
Vivek Murthy, M.D., for a second tour of duty as surgeon general
Rochelle Walensky, MD, Harvard professor, as CDC director
Marcella Nunez-Smith, MD, Yale Professor, as COVID-19 Equity Task Force Chair
Jeff Zients, Deputy OMB Director for Management in Obama Administration, as Covid-19 czar.
Anthony Fauci, MD, as Coordinator of COVID-19 response and Counselor to the President
Sidebar — Still waiting for FDA Commissioner appointment
Added Cathie McQuiston, AFGE Deputy GC, to the OPM review team
Tomorrow December 10 is the date set for the FDA Vaccines and Related Biological Products Advisory Committee virtual meeting on the Pfizer-BioNTech emergency use authorization application for its COVID-19 vaccine. The CDC’s Advisory Committee on Immunization Practices will meet on Friday December 11 and vote on Sunday December 13 per Reuters. “
Dr. William Schaffner, an infectious disease expert and non-voting member of the CDC’s ACIP, said the gap between the two ACIP meetings will allow the FDA time to draft and issue an emergency use authorization (EUA) before the ACIP vote. That schedule could change, however, if FDA advisers have questions or request more data [tomorrow], he said.
authorized LabCorp’s Pixel COVID-19 Test Home Collection Kit for use by any individual 18 years and older without a prescription. This product, which is authorized as the first COVID-19 direct-to-consumer (non-prescription) test system, allows an individual to self-collect a nasal swab sample at home and then send that sample for testing to LabCorp. Positive or invalid test results are then delivered to the user by phone call from a health care provider. Negative test results are delivered via email or online portal.
This home sample collection kit can be purchased online or in a store without a prescription. It is intended to enable users to access information about their COVID-19 infection status that could aid with determining if self-isolation (quarantine) is appropriate and to assist with health care decisions after discussion with a health care professional.
“This is the first kit for consumers to self-collect a nasal sample for COVID-19 in their home that does not require a prescription,” said Jeff Shuren, M.D., J.D., director of FDA’s Center for Devices and Radiological Health. “While many home collection kits can be prescribed with a simple online questionnaire, this newly authorized direct-to-consumer collection kit removes that step from the process, allowing anyone to collect their sample and send it to the lab for processing.”
Blue Cross and Blue Shield is calling on payers to bolster vaccination rates by expanding access to care, connecting with members through digital platforms, hosting free flu vaccine clinics, and utilizing data to target support for at-risk communities The effort comes in response to a drastic decrease in the number of vaccinations this year, compared with 2019 data.
The Trump administration made a $916 billion coronavirus relief offer to Democrats, opening yet another front in the multi-track effort to reach an agreement in talks that rank-and-file lawmakers have been leading in the final weeks of the year. The proposal, announced in a brief statement by Treasury Secretary Steven Mnuchin, came after Democrats rejected an effort by Senate Majority Leader Mitch McConnell (R., Ky.) to narrow the scope of a coronavirus relief bill by excluding aid for hard-hit state and local governments prioritized by Democrats and liability protections sought by Republicans.
The President’s proposal reportedly includes $600 per person direct payments. The FEHBlog will be surprised if the COVID-19 relief bill negotiations are unsuccessful, but it would be hardly be the first time that Congress surprises the FEHBlog.
Also according the Wall Street Journal, the House of Representatives tonight passed the FY 2021 National Defense Authorization Act by a veto proof 335-78 margin. As the FEHBlog noted last week this bill includes goodies for federal employees. Federal News Network identifies policy winners and losers in this must pass bill which now goes over to the Senate.
Federal News Network columnist Mike Causey touts the FEHBlog’s personal favorite health plan design the high deductible health plan with health savings account (“HSA”). Mr. Causey aptly describes the HSA as a “Roth IRA on steroids” because and HSA is triple tax favored — tax exempt on the way in and out and grows tax free while in the account. The Federal Benefits Open Season ends on Monday December 14.
The FDA has released its internal review documents ahead of the closely watched COVID-19 vaccine advisory committee meeting scheduled for Thursday [December 10] —and they bode well for Pfizer and partner BioNTech’s prospects for securing a quick emergency use authorization (EUA). The FDA meeting briefing, published (PDF) on Tuesday, confirmed the efficacy and safety profile of Pfizer and BioNTech’s BNT162b2, reiterating that the shot was 95% effective at preventing COVID-19 after two doses with no serious safety concerns.
The Moderna vaccines turn before this panel occurs one week later on December 17.
Hospitals are readying for Jan. 1, [2021] when they expect they will have to publicly disclose the negotiated prices they reach with insurers for services performed inside their facilities — barring any intervention from a federal appeals court. [Such intervention in the FEHBlog’s humble opinion, is highly unlikely.]
The policy requires hospitals to share two streams of information. First, hospitals will have to share a machine-readable format of its negotiated prices with every insurer and every insurance product — a sizable pool of information.
Then they will also have to prepare a list of 300 “shoppable services.” A total knee replacement would be a good example. It’s a procedure a consumer likely has time to plan and prepare for, unlike an emergency surgery due to an accident or failing health. The idea is to provide the price information so consumers can shop around for the best deal.
The FEHBlog attended the second day of the American Bar Association’s Washington Health Law Summit (“WLS”). It’s worth noting that every panelist (six or seven in total) who has opined on the outcome of the Supreme Court’s California v. Texas case on the ACA’s constitutionality shares the FEHBlog’s opinion that the Supreme Court will preserve the ACA expect perhaps for the individual mandate which Congress effectively repealed in 2017.
The FEHBlog listened to three hours of discussion about behavioral telehealth and artificial intelligence during the WLS. It turns out that two types of healthcare AI exist admin AI and operational AI. AI can be assistive to the user’s decision making or can yield autonomous decisions. The Food and Drug Administration oversees the AI devices and the operational devices typically are used with imaging procedures. The FDA has approved two autonomous operational AI devices. The radiologists however has doubts about those devices.
The most interesting thing that the FEHBlog heard during this discussion was a remark from a Doctors on Demand speaker that telehealth companies are facing challenges in filling provider slots for psychiatrists and psychologists because of the enormous demand for mental health telemedicine. That’s a good thing. He noted that the explosion in telehealth use in 2020 is principally due to the government permitting a doctor or psychiatrist licensed in state A to treat a telehealth patient in state B.
The other speakers added that healthcare providers were quick to pick up on telehealth due to the licensing flexibilities and Medicare equivalent payments. They expressed their understanding that telehealth changes the personal dynamics between doctors and patients. Patients feels more in charge in a tele heath setting than they do in the office setting, and providers get social determinants of health data from seeing where the patient lives.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.