Friday Stats and More
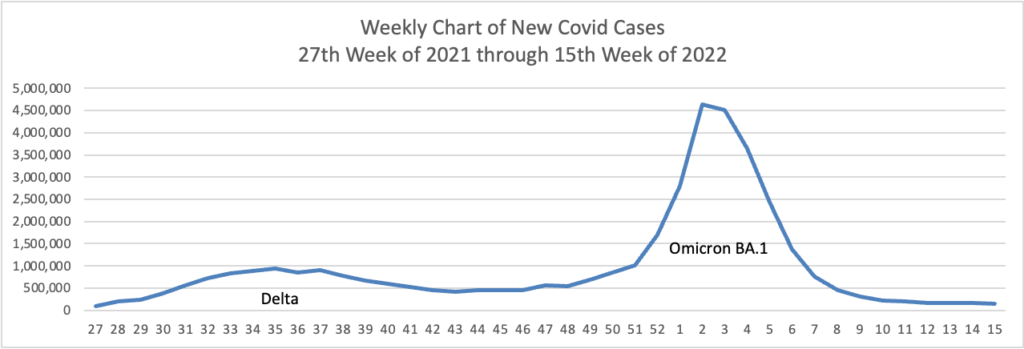
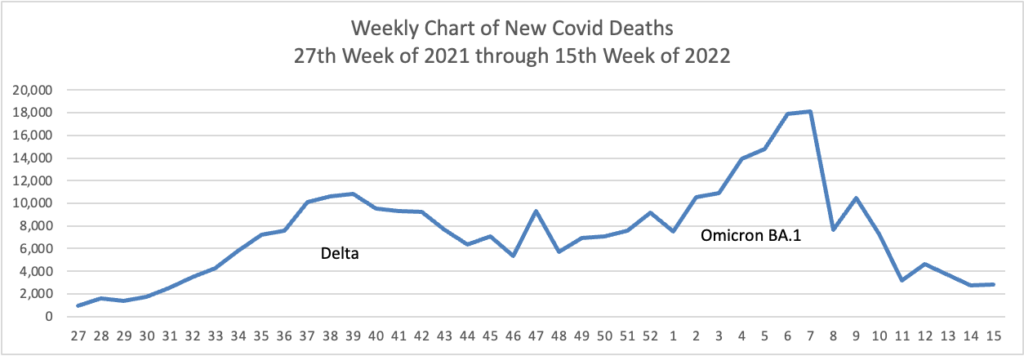
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first day of the month, here are the FEHBlog’s weekly charts of new Covid cases and deaths
Here is a link to the CDC’s weekly review of COVID statistics. Among those statistics are the following:
New Hospital Admissions
The current 7-day daily average for April 6–April 12, 2022, was 1,446. This is a 1.3% increase from the prior 7-day average (1,427) from March 29–April 4, 2022.
Here’s the FEHBlog’s weekly chart of Covid vaccinations distributed and administered from the beginning of the Covid vaccination era to the latest week ending last Wednesday, April 13.
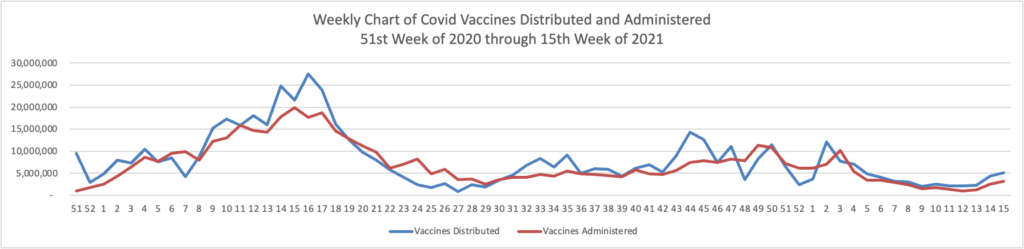
For the second week in a row, Covid vaccines distributed and administered have increased materially.
The CDC’s principal point in this week’s Covid statistical review is the following:
Throughout the COVID-19 pandemic, many people have delayed or avoided medical care, including routine, urgent, and emergency care. If it’s something you’ve neglected, it’s time to jump back in—consider putting “get a checkup” on top of your to-do list, especially if you’re at risk for heart disease. Regular checkups provide the opportunity to prevent, screen for, and manage chronic conditions, and to get routine vaccinations.
The FEHBlog agrees that the best step a person can make on the road to a healthy life is to establish a relationship with a primary care doctor.
In other Omicron and siblings news —
MedPage Today informs us
The FDA granted an emergency use authorization (EUA) to the first COVID-19 test that can detect the virus in breath samples, the agency announced on Thursday.
Dubbed the InspectIR COVID-19 Breathalyzer, the test uses gas chromatography-mass spectrometry to rapidly detect volatile organic compounds associated with SARS-CoV-2. Patients breathe into a disposable straw on the device — which is about the size of a piece of carry-on luggage, according to the agency — and results are returned in less than 3 minutes. The test is intended for healthcare settings where samples can be collected and analyzed, such as mobile testing sites, doctor’s offices, and hospitals.
Cool.
Kaiser Health News tells us
The federal “test-to-treat” program, announced in March, is meant to reduce covid hospitalizations and deaths by quickly getting antiviral pills to people who test positive. But even as cases rise again, many Americans don’t have access to the program.
The program allows people with covid symptoms to get tested, be prescribed antiviral pills, and fill the prescription all in one visit. The federal government and many state and local health departments direct residents to an online national map where people can find test-to-treat sites and other pharmacies where they can fill prescriptions.
But large swaths of the country had no test-to-treat pharmacies or health centers listed as of April 14. * * *
Even people who regularly see a doctor may be unable to get a prescription in time, and that’s where the program comes in. Before the pandemic, 28% of Americans didn’t have a regular source of medical care, with rates even higher for Black and Hispanic Americans.
See above re PCPS and no bueno.
The article adds
Truepill, a company that provides telehealth and pharmacy technology, offers online covid assessments through its website findcovidcare.com * * *. The company has filled more than 10 million prescriptions in the past five years.
The service, available in all 50 states and Washington, D.C., costs $25 to $55. Though insurance isn’t accepted, the cost is comparable to insurance copays for in-person doctor appointments. Prescriptions can be sent to a local pharmacy for no additional charge or shipped to a home overnight via FedEx for a $20 fee.
It’s always good to have a Plan B.
From the FEHB front, OPM issued a final, final rule concerning a Consolidated Appropriations Act 2021 provision extending the opportunity for tribal employers to enroll employees at certain tribal schools to join the FEHB Program.
From the Social Determinants of Health Front, Fierce Healthcare calls to our attention
a Northeast Business Group on Health guide for employers looking to tackle obesity and diabetes through a racial lens. “Obesity, Diabetes and Health Equity: What Employers Can Do” lays out a step-by-step approach. Key among them is embedding health outcomes within other diversity, equity and inclusion efforts. Another big recommendation is to build benefits to address obesity and diabetes that are based in clinical best practices.
In the FEHBlog’s view, OPM’s 2023 call letter asks carriers to address member obesity issues in this manner.
From the Rx coverage front, the Wall Street Journal reports
After Covid-19, vaccine makers’ next big target is a respiratory virus that kills up to 500 children a year nationwide and has been among the leading causes of U.S. hospitalizations for decades.
The respiratory syncytial virus, or RSV, infects nearly everyone at some point, causing mild, cold-like symptoms for most people. But it can lead to serious health problems such as difficulty breathing and pneumonia for infants and older adults.
Now several drugmakers including Pfizer Inc., Johnson & Johnson, Moderna Inc. and GlaxoSmithKline PLC are testing shots that infectious-disease specialists say show promise at safely preventing RSV disease. Initial development of most of these vaccines predated the current pandemic, but the rapid success in finding effective Covid-19 vaccines has energized the RSV effort, according to analysts.
Good luck.
From the federal government front
- Meritalk provides a Who’s Who in implementing the President’s Management Agenda. The article explains “As the Office of Management and Budget’s (OMB) effort to transform the President’s Management Agenda from a list of goals into actionable policy steps gathers steam, OMB is fleshing out its list of Federal agency officials who are taking on leadership roles not only for the three major PMA pushes but for numerous strategic goals within each of them.” The OPM Director Kiran Ajuha is one of three senior federal executives in charge of the PMA’s workforce issues.
- Federal News Network offers an interview with the Postmaster General Louis Dejoy.