From Capitol Hill, Fierce Healthcare points out four legislative items that providers should be tracking for the remainder of this year.
From the Omicron and siblings front, the Washington Post reports
Cold weather favors the coronavirus. But as summer gives way to fall, infectious-disease experts are guardedly optimistic that the spread of covid-19 this autumn and winter won’t be as brutal as in the previous two years of the pandemic.
Coronavirus scenarios from multiple research teams, shared in recent weeks with federal officials, foresee stable or declining hospitalizations in early fall.The scenarios show the possibility of a late-fall surge. A new variant remains the biggest wild card. But several factors — including the approval this week of reformulated boosters and the buildup of immunity against the latest strain of the virus — could suppress some of the cold-season spread, experts say.
In related news, the Wall Street Journal informs us
U.S. health authorities plan to recommend that people get Covid-19 boosters once a year, starting with the new shots now rolling out, a shift from their current practice of issuing new advice every several months.
The annual cadence would be similar to that of flu shots, White House officials said Tuesday, though elderly people and those with weakened immune systems may need more frequent inoculations.
A shift to annual Covid-19 boosters would be a departure from current practice and comes after many people in the U.S. have ignored calls to get a first or second booster, partly due to fatigue with repeat inoculations.
“Barring any new variant curveball,” said White House coronavirus coordinator Ashish Jha, “for a large majority of Americans, we are moving to a point where a single annual Covid shot should provide a high degree of protection all year.”
A very sensible approach, indeed!
From the healthcare business front, Healthcare Dive tells us
Amazon and One Medical said Friday that antitrust regulators want more information about the online retailer’s proposed $3.9 billion acquisition of the primary care group.
The Federal Trade Commission sent a second request for information on Friday, One Medical said in a filing with the U.S. Securities and Exchange Commission.
A second request from the FTC means the two cannot move forward with the deal “until the companies have substantially complied with the additional investigatory request,” according to the FTC.
Amazon and One Medical will “promptly respond” to the second request, the primary care group said in the SEC filing.
Drug Channels surveys the upcoming Humira price war as biosimilar competitors take the field.
CMS posted new information about available group health plan defenses to CMS contractor assertions that the GHP has failed to properly coordinate its benefits with Medicare.
Beckers Payer Issues offers expert opinions on the impact of the transparency in coverage rule on consumerism now that the three machine-readable files of health plan pricing data have been posted for two months. For example, “Neil Mayle is the founder and president of Visible Charges, a Cambridge, Mass.-based company that provides clients with curated datasets of both payer- and provider-negotiated service prices. * * * ‘I think we’ve gone from nothing to a lot,’ Mr. Mayle said. ‘We haven’t gone to perfect.'” Of course, it was only the first of three stages in transparency in coverage rule disclosures.
The FEHBlog noticed today these CMS and DOL fact sheets on the No Surprises Act which are worth a gander.
Senate Democrats are growing more anxious over maverick Sen. Kyrsten Sinema’s (D-Ariz.) five-day silence on a sweeping proposal to reform the tax code, tackle climate change and reduce the federal deficit.
Democratic lawmakers are privately worried that Sinema’s not happy about being left out of the negotiations between Senate Majority Leader Charles Schumer (D-N.Y.) and centrist Sen. Joe Manchin (D-W.Va.), which resulted in a surprise announcement last week of a major deal.
Govexec.com reports on the Republican response to the Senate Appropriations Committee’s release of its twelve fiscal year 2023 appropriations bills last week.
From the Medicare front, Fierce Healthcare informs us
The Biden administration finalized a 4.3% bump for inpatient payments for the federal fiscal year 2023, an increase compared to the 3.2% that was originally proposed back in April.
The Centers for Medicare and Medicaid Services released on Monday the final Inpatient Prospective Payment System (IPPS) and Long-Term Care Hospital Prospective Payment System rule that updates payments to hospitals. The rule also details health equity quality measures hospitals must now meet for participation in the Inpatient Quality Reporting program.
Here’s a link to the CMS fact sheet on this final rule.
Revcycle Intelligence tells us that last week “CMS released FY23 final rules for hospice providers,inpatient psychiatric facilities, and inpatient rehabilitation facilities. The final rules for fiscal year 2023 include a 3.8% payment increase for hospice providers, 2.5% increase for inpatient psychiatric facilities, and 3.2% boost for inpatient rehabilitation facilities.
Also, last week, CMS released the FY 2023 final rules for skilled nursing facilities. The rule represents a 2.7% payment increase for SNFs.
Fierce Healthcare adds “CMS said Friday [July 29] that it expects the average premium to decrease to $31.50 in 2023, or about 1.8% from the 2022 rate of $32.08.
From the healthcare quality front, the National Committee for Quality Assurance released its Measurement Year 2023 HEDIS and CAHPS guidelines today. NCQA made publicly available a list of adds, drops and other significant changes for MY 2023.
From the U.S. healthcare business front, Bloomberg reports
Labcorp, a diagnostics and laboratory company, is spinning off its clinical trials division into a separate publicly traded company.
Labcorp will house the company’s existing global laboratory business while the new company will manage clinical trials for drug companies. Management said in a release Thursday [July 28] that this structure will allow each division more flexibility to grow within their individual markets.
From the post-Dobbs front, Healthcare Dive tells us
Abortion access nonprofit Just the Pill plans to build a fleet of mobile clinics offering mobile procedural abortion “for the first time in U.S. history,” the nonprofit said. * * *
The group currently operates two mobile clinics in Colorado and plans to build out its network of vans and deploy them in states where abortion is legal but surrounding states have banned the procedure, such as New Mexico, Pennsylvania and Illinois.
“Our mobile clinics will travel to parts of these states based on where the need is greatest,” Julie Amaon, medical director of Just The Pill, told Healthcare Dive. * * *
Mobile health clinics have been held up as an avenue to cut costs and expand healthcare access, especially in underserved or marginalized communities. One 2009 Boston study found that a mobile health clinic, The Family Van, had a return on investment of $36 for every $1 invested in the program. Mobile clinics can also provide primary and preventative care, an important feature given that many regions in the U.S. lack healthcare access.
From the wellness front, Morning Consult provides advice on offering wellness services to younger employees.
While benefits like annual raises and an employee assistance program (EAP) with appointment limits have been alluring, these perks are now expected by many Millennial and Gen Z employees, who will soon make up 75% of the U.S. workforce.
Improving hiring and retention for the shifting workforce starts with understanding the core values that drive younger generations to join, or leave, organizations in the first place – and that’s health and mental well-being, as a whopping 83% of employees place their benefits as a main deciding factor in whether they will stay at their current job.
As a baby boomer, the FEHBlog prefers to refer to the younger crowd as Zoomers over Gen Z.
From the medical research front —
Medscape reports “A simple blood test that looks for a combination of specific RNA snippets may become a novel way to screen for early-onset colorectal cancer, suggests a new study published online in Gastroenterology.”
“The point would be to use this test as a routine part of annual healthcare, or for people in high-risk families every 6 months,” study senior author Ajay Goel, PhD, MS, chair of the Department of Molecular Diagnostics and Experimental Therapeutics at the City of Hope Comprehensive Cancer Center, Duarte, California, told Medscape Medical News.
“It’s affordable, it can be done easily from a small tube of blood, and as long as that test stays negative, you’re good,” Goel said, because even if patients miss a test, the next one, whether it’s 6 months or a year later, will catch any potential cancer.
A study published this week in Nature Communications shows that an automated clinical decision support tool for genetic disease diagnosis and treatment can provide accurate results and disease management guidance within 13.5 hours.
The tool, known as Genome-to-Treatment (GTRx), is a virtual disease management system that integrates whole genome sequencing to provide diagnostics and guidance for 500 diseases, according to a press releasediscussing the study’s findings. The study was completed in collaboration with multiple organizations, vendors, and health systems.
The study states that the 7,200 genetic disorders currently known to medical science result in high levels of morbidity and mortality in children, specifically in neonatal, pediatric, and cardiovascular patients. Approximately 140 million children worldwide suffer from rare genetic diseases, and experts estimate that 30 percent of them will not survive until their 5th birthday.
From the miscellany department, STAT News asks why monkeypox does not have a new name yet. The FEHBlog wonders if monkeypox’s name is changed, then what’s next chickenpox? swine flu?
A bill that would cap out-of-pocket insulin costs for the insured at $35 per month remains in limbo as the Congressional Budget Office told the two Senate sponsors of the bill that it will likely increase net prices for insulin, and will increase premiums for commercial health insurance and Medicare Part D.
The comments from the CBO may spell the end for the bill, which is effectively a Band-Aid for a segment of the pharma market that has ballooned in recent years, driving many to ration their life-saving drug.
“Spending for insulin and other pharmaceutical products would increase, CBO estimates, because overall medication use would increase in response to lower cost-sharing requirements,” CBO director Phillip Swagel wrote to Sens. Jeanne Shaheen (D-NH) and Susan Collins (R-ME) on Friday. “Some use of insulin might also shift to newer and more expensive insulin products. Increased spending for pharmaceutical products would result in increased spending for health care overall.”
Democrats are closer than ever before to finally achieving a goal they’ve been pursuing for nearly two decades — allowing Medicare to negotiate prescription drug prices. Skeptical lawmakers seem to be on board; the bill text is already under review by the Senate’s rules referee. Congressional leadership and the White House have come up with a plan to barrel toward a vote that could come as soon as next week.
Drugmakers, in turn, are intensifying their opposition efforts.
Charley Ding spent weeks early in the pandemic intubating patients sick with Covid-19. The 42-year-old anesthesiologist in South Barrington, Ill., said he has since watched most of the doctors and nurses he works with get infected at some point.
But he has never gotten Covid-19, he said. “It’s probably a combination of being careful, maybe being blessed with a good immune system,” he said. “But also just luck.”
Dr. Ding is a member of a shrinking club of people who are pretty sure they have never been infected with SARS-CoV-2, the virus that causes Covid-19. Geneticists and immunologists are studying factors that might protect people from infection, and learning why some are predisposed to more severe Covid-19 disease.
For many, the explanation is likely that they have in fact been infected with the virus at some point without realizing it, said Susan Kline, professor of medicine at the University of Minnesota Medical School. About 40% of confirmed Covid-19 cases are asymptomatic, according to a meta-analysis published in December in the Journal of the American Medical Association.
More than two years into the pandemic, most people worldwide have likely been infected with the virus at least once, epidemiologists said. Some 58% of people in the U.S. had contracted Covid-19 through February, the Centers for Disease Control and Prevention has estimated. Since then, a persistent wave driven by offshoots of the infectious Omicron variant thas kept daily known cases in the U.S. above 100,000 for weeks.
As someone who is a member of Dr. Ding’s shrinking club, the FEHBlog thinks that he may have had Covid at some point and in any event, it’s a matter of time before officially contracts it. Covid is gaining similarity to its cousin the common cold.
The FEHBlog has moved his residence inside the Capital Beltway to Dripping Springs, Texas. His Texas residence has a home office. He has come back to work at his DC law firm this week. When working in DC, he stays at a hotel next to his office building. All of this has cut into his commuting time when he listened to Russ Robert’s Econtalk. This evening he traveled up to have dinner with one of his sons outside Baltimore. This allowed him to listen to the July 18 episode of Econtalk during which Russ Roberts discussed Covid with Dr. Vinay Prasad of the University of California San Francisco. Their conversation is very insightful into the public health aspects of the Covid pandemic. It’s worth a listen or read the transcript on the website.
From the public health front, the Department of Health and Human Services announced
Today, the Centers for Medicare & Medicaid Services (CMS) unveiled its Maternity Care Action Plan to support the implementation of the Biden-Harris Administration’s Blueprint for Addressing the Maternal Health Crisis. The action plan takes a holistic and coordinated approach across CMS to improve health outcomes and reduce inequities for people during pregnancy, childbirth, and the postpartum period. CMS’ implementation of the action plan will support the Biden-Harris Administration’s broad vision and call to action to improve maternal health.
“Strengthening maternal health is key to strengthening the health and wellbeing of communities across America,” said HHS Secretary Xavier Becerra. “At HHS, we are taking unprecedented action to advance the Biden-Harris Administration’s vision to improve maternal health and tackle disparities, and I’m proud of the bold action plan CMS has laid out to contribute to our goals. Today is just the beginning: we will tirelessly work to make sure all mothers get the care and support they need.”
Through the action plan, CMS Administrator Chiquita Brooks-LaSure also encouraged industry stakeholders – including health care facilities, insurance companies, state officials, and providers – to consider key commitments the private sector can make to improve maternal health outcomes. Industry can submit proposed commitments at http://cms.gov/maternalhealthcommitments .
From the U.S. healthcare front, Healthcare Dive tells us
The Mayo Clinic earned the No. 1 spot for a seventh straight year in U.S. News & World Report’s best hospitals ranking published Tuesday. Cedars-Sinai Medical Center, NYU Langone Hospitals and the Cleveland Clinic followed next, with Johns Hopkins Hospital and UCLA Medical Center tied in fifth place.
In the specialty rankings, University of Texas MD Anderson Cancer Center was named best in cancer, Cleveland Clinic was first in cardiology and heart surgery, and NYU Langone Hospitals led in neurology and neurosurgery.
U.S. News added three service areas of evaluation this year, for ovarian, prostate and uterine cancer surgeries. The publication also introduced “home time” as an outcome measure in certain ratings, reflecting patients’ preference for recovering at home.
Becker’s Health IT looks at the Amazon – One Medical deal from the perspective of Amazon v. Optum.
From the U.S. healthcare business front, Fierce Healthcare reports
In its latest earnings results, [health insurer Centene] posted a $172 million loss in the second quarter, still beating the Street and slimming its losses compared to the prior year’s quarter. In the second quarter of 2021, Centene reported a $535 million loss, according to its earnings report released Tuesday morning. * * *
The company added about 200,000 members in the second quarter, reaching 26.4 million in total membership. That’s up by more than one million from the second quarter of 2021, when the insurer reported 24.7 million members.
“Our strong second quarter results reflect the consistency of Centene’s product performance,” Centene CEO Sarah London said in a statement. “The second quarter reflects continued execution on our Value Creation Plan with tangible actions and results, providing an excellent foundation from which we will continue to build over the next couple of years.”
From the reports and studies (tidbits?) department —
It’s payers, not providers, that American turn to when seeking out pricing information for healthcare services, according to a survey on price transparency.
The poll, conducted by YouGov on behalf of AI for healthcare operations company AKASA, highlights the need for both insurers and providers to follow pricing regulations for the sake of the patient experience.
Of the 2,026 adults surveyed nationally in March, just 36% indicate they have researched prices for services, of which 60% say they would look to their insurance company for pricing information.
When seeking out information through a payer, 44% would look on the insurer’s website and 29% would call their insurer.
A majority of those who receive health insurance through their employer-provided plan said they are more satisfied with the coverage they receive through work than they are with the current health insurance system overall.
That was one of the key takeaways from research conducted by Locust Street Group and presented at a webinar by America’s Health Insurance Plans. The research was part of AHIP’s Coverage@Work campaign, which aims to educate policymakers and the public about the value of employer-provided coverage.
The survey showed that although 54% of the 1,000 adults surveyed said they are satisfied with the current health system overall, 67% said they were satisfied with the coverage they receive through their employer.
What makes someone satisfied with their coverage? The top three reasons given were:
* Affordability – 45%
* Comprehensive coverage – 45%
* Choice of providers – 44%
Other factors that rounded out the list of reasons for being satisfied included: free preventive services, consistency, customer service, the ability to receive care locally, wellness incentives and innovation.
The Washington Post reports “A congressional deal for billions of dollars in additional coronavirus funding appeared all but dead Thursday [June 16] after Senate Republicans accused the White House of being dishonest about the nation’s pandemic funding needs.” The FEHBlog expects we have not heard the end of this issue.
The Centers for Disease Control and Prevention recommended that children as young as 6 months receive newly authorized Covid-19 shots, the final step to making the vaccines available.
On a related note, Precision Vaccinations tells us
The U.S. Centers for Disease Control and Prevention (CDC) reported today the number of pneumonia-related fatalities continues to outpace both COVID-19 and Influenza. * * *
In the USA, common causes of viral pneumonia are influenza, respiratory syncytial virus, and SARS-CoV-2 viruses. A common cause of bacterial pneumonia is Streptococcus pneumoniae.
The good news is pneumonia is a vaccine-preventable disease, and the U.S. FDA has approved two types of pneumococcal vaccines, PCV13, and PPSV23. * * *
Unfortunately, the CDC’s data shows that in 2020, the percentage of adults who received a pneumococcal vaccination was just 25.5%.
FEHB plans may want to focus on this issue given the Program’s demographics.
From the U.S. healthcare front, the American Medical Association provides background on its freshly inaugurated President, Dr. Jack Resneck, Jr., and gives an account of Dr. Resneck’s inaugural address. Good luck, Dr. Resneck.
A growing number of Senate Democrats say they’re ready to take a tough vote on an amendment to keep the Title 42 health order in place at the U.S.-Mexico border if that’s what’s needed to move a stalled COVID-19 relief package.
Senate Majority Leader Charles Schumer (D-N.Y.) has held the bill from the floor because Republicans are insisting on voting on a bipartisan amendment to overrule the Biden administration’s decision to lift Title 42, a pandemic order that has stopped thousands of immigrants from entering the country on asylum claims. * * *
Without giving in to the Republicans’ demand for a vote on the hot-button issue of securing the border, COVID-19 relief could be stalled until after the November election.
The amendment is expected to fail but it’s a tough vote for vulnerable Senate Democrats.
More likely, in the FEHBlog’s view, the Majority Leader is waiting until the Title 42 health order is lifted later this month to see what happens.
Following the recommendation Thursday, many of the nation’s doctors, pharmacies and other vaccination sites are expected to begin offering the extra doses to the 28 million U.S. children in the age group.
The shots are to be given five months after the second dose. The extra dose is one-third the amount that those 12 years old and above receive.
Also Thursday, the CDC said it was strengthening its recommendation that people 12 years and older who are immunocompromised, or who are 50 and older, should receive a second booster dose at least four months after their first.
This means that health plans must start covering the booster with no member cost-sharing pursuant to ACA FAQ 50.
“We are ready from a manufacturing standpoint,” Moderna Chief Executive Stéphane Bancel said during a virtual appearance Thursday at The Wall Street Journal’s Future of Everything Festival.
The FDA/CDC decision is expected next month.
In other virus news, STAT News interviewed a top CDC expert on monkeypox. From the FEHBlog’s standpoint, the key takeaway is that monkeypox is not Covid.
I think we can take away a lot from what we know about monkeypox in Congo Basin and in West Africa. Even if human-to-human transmission is documented, it is generally documented among very close contacts. So family members, people taking care of ill patients. Or health care providers.
In funding news, the Department of Health and Human Services announced today a $1.5 billion funding opportunity under the State Opioid Response
SOR grant program provides formula funding to states and territories for increasing access to FDA-approved medications for the treatment of Opioid Use Disorder (OUD), and for supporting prevention, harm reduction, treatment, and recovery support services for OUD and other concurrent substance use disorders (SUD). The SOR program also supports care for stimulant misuse and use disorders, including for cocaine and methamphetamine. The SOR program helps reduce overdose deaths and close the gap in treatment needs across America by giving states and territories flexibility in funding evidence-based practices and supports across different settings to meet local community needs.
From the miscellany department
Today “the U.S. Office of Personnel Management (OPM) released guidance regarding the implementation of EO 13932; Modernizing and Reforming the Assessment and Hiring of Federal Job Candidates. OPM’s guidance represents a major step towards the federal government’s adoption of skills-based hiring practices and is an important innovation in federal hiring, which has historically relied on education and candidate self-assessments as a proxy for a candidate’s ability to perform in a job. This new approach helps hiring managers recognize and value skills regardless of where they were acquired, whether in a formal degree program, on the job, or on one’s own.”
Employee Benefit News identifies the ten most popular mental health and wellness apps.
Benefits consultant Tammy Flanagan discusses federal employee life insurance benefits in Govexec.
Health Payer Intelligence reports that CMS has updated the Medicare.gov website “to include new features such as highlighting pages that answer popular questions and spotlighting key steps that consumers should take related to Medicare coverage.”
From the Omicron and siblings front, Fortune Well explores earlier pandemics for similarities to our current one.
As U.S. COVID czar Dr. Anthony Fauci and colleagues pointed out in a 2009 New England Journal of Medicine article, “It is not generally appreciated that descendants of the H1N1 influenza A virus that caused the catastrophic and historic pandemic of 1918–1919 have persisted in humans for more than 90 [now 100] years and have continued to contribute their genes to new viruses, causing new pandemics,” including the 2009 H1N1 “swine flu.”
“We are living in a pandemic era that began around 1918,” they wrote 13 years ago—long before the advent of COVID-19.
“They change and hopefully they adapt and behave,” Brüssow said. “But there are still some escapes, and we might see a return with higher virulence. Vigilance is indicated.”
Pfizer Inc. expects demand for its Covid-19 antiviral drug to increase as governments return to replenish their supplies and seek to thwart surges as the pandemic virus continues to evolve.
The treatment, a pill called Paxlovid, brought in $1.5 billion in sales during Pfizer’s first quarter, while its vaccine totaled $13.2 billion, reflecting the need for tools to combat the virus despite a slowdown in cases and a growing sense of life trying to return to normal.
The company said Tuesday it is on track to deliver between $98 billion and $102 billion in revenue for the year, with $32 billion coming from its Covid-19 vaccine Comirnaty and $22 billion from Paxlovid.
“We remain bullish on Paxlovid” said Chief Financial Officer Frank D’Amelio on a call discussing earnings with analysts. “The rhythm of that product looks very good.”
Biogen is replacing CEO Michel Vounatsos, the company said Tuesday, ending a five-year tenure in which he presided over the disastrous approval and rollout of its Alzheimer’s treatment, Aduhelm.
The company also said it is “substantially eliminating” all spending on Aduhelm just 10 months after securing U.S. approval — a concession from the struggling biotech that the drug had become a financial liability following a Medicare decision to restrict patient access and payment.
From the Affordable Care Act front, Health Affairs Forefront features the third and final part of Katie Keith’s series on the final 2023 notice of benefit and payment parameters. The third part discusses changes to the ACA marketplace’s risk adjustment program.
From the No Surprises Act, the FEHBlog had understood that the NSA regulators planned to release a final rule on the NSA’s arbitration process, replacing the interim final rule, this month. However, a Justice Department filing with the U.S. Court of Appeals for the Fifth Circuit submitted late last week states, “the Departments expect to issue a final rule early this summer that will supersede the portions of the interim final rule that Plaintiffs [in the Texas Medical Association case] challenged.” No wonder then that the final rule has not been presented yet to OMB’s Office of Information and Regulatory Affairs for its required review before publication in the Federal Register.
Agencies’ hiring efforts for the Bipartisan Infrastructure Law (IIJA) are “foot to the pedal,” OPM Director Kiran Ahuja said in an exclusive interview with Federal News Network.
The surge includes filling 3,000 of those new positions over the first six months after President Joe Biden signed the bill into law.
Ahuja has frequently spoken about her goals to attract more early-career workers to federal service. The BIL gives OPM another chance to do just that.
FedSmith identifies four personal budget factors Federal retirees must anticipate. One of those factors is our beloved FEHBP.
The CDC offers ten tips for coping with diabetes distress.
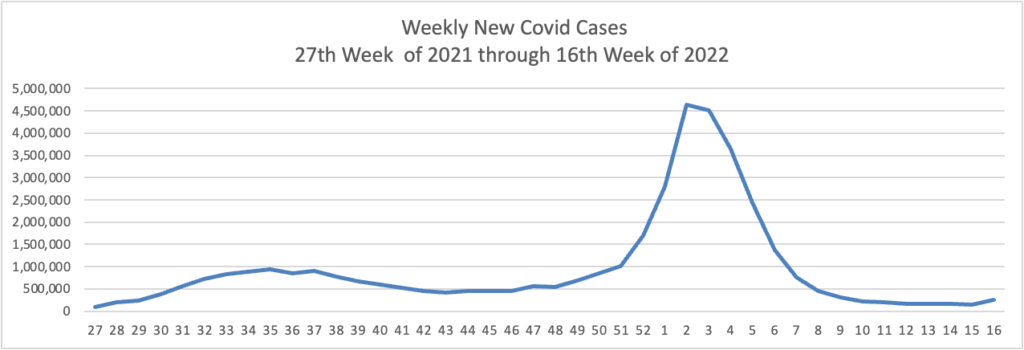
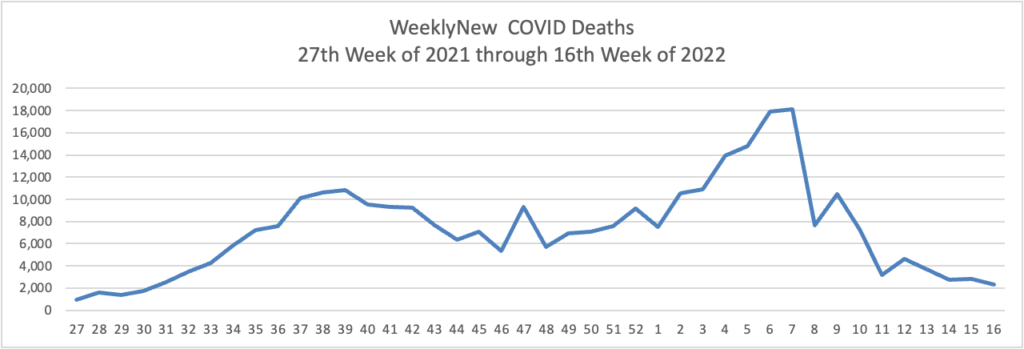
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first day of the week, here are the FEHBlog’s latest weekly charts of new Covid cases and deaths.
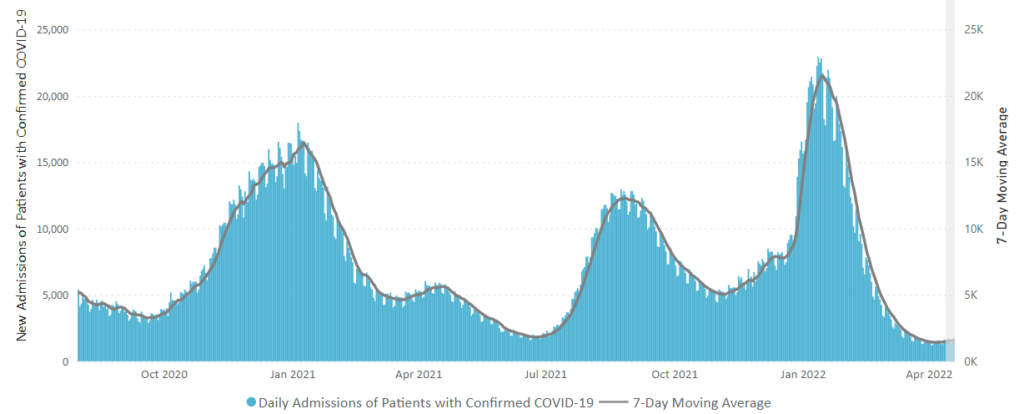
Because David Leonhardt in the New York Times recommends keeping an eye on Covid hospital admissions here is the CDC’s latest chart
The weekly new cases and death chart start in the middle of 2021 when we hit all time lows in new cases. Although our new cases total for the past week was 3 times week 27 in 2021, the new hospitalizations level is lower. That’s good news.
The CDC’s weekly review of its Covid stats adds
Currently, there are 39 (1.21%) counties, districts, or territories with a high COVID-19 Community Level, 231 (7.17%) counties with a medium Community Level, and 2,954 (91.63%) counties with a low Community Level. This represents a slight (0.78%) increase in the number of high-level counties, a small (+1.67%) increase in the number of medium-level counties, and a corresponding (−2.45%) decrease in the number of low-level counties. Twenty-five (44.64%) of 56 jurisdictions had no high- or medium-level counties this week.
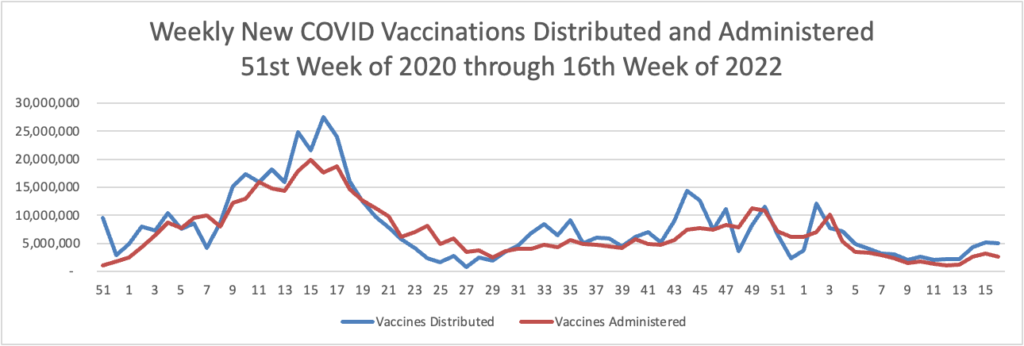
Here’s the FEHBlog’s latest weekly chart of Covid vaccinations distributed and administer from the beginning of the COVID vaccination era to the 16th week of 2022.
New vaccinations remain above 2 million per week.
From the Medicare front, the Centers for Medicare Services announced today a proposed rule that would create five new special Medicare enrollment periods.
An SEP forIndividuals Impacted by an Emergency or Disaster that would allow CMS to provide relief to those beneficiaries who missed an enrollment opportunity because they were impacted by a disaster or other emergency as declared by a Federal, state, or local government entity.
An SEP for Health Plan or Employer Error that would provide relief in instances where an individual can demonstrate that their employer or health plan materially misrepresented information related to enrolling in Medicare timely.
An SEP for Formerly Incarcerated Individuals that would allow individuals to enroll following their release from correctional facilities.
An SEP to Coordinate with Termination of Medicaid Coverage that would allow individuals to enroll after termination of Medicaid eligibility.
An SEP for Other Exceptional Conditions that would, on a case-by-case basis, grant an enrollment period to an individual when circumstances beyond the individual’s control prevented them from enrolling during the IEP, GEP or other SEPs.
These “SEPs that would provide individuals who meet certain exceptional conditions and who missed a Medicare enrollment period an opportunity to enroll without having to wait for the GEP and without being subject to a [Part B] late enrollment penalty.”
UnitedHealth Group subsidiary Optum has quietly acquired at least two independent primary care groups in Oregon, according to The Lund Report.
Optum has purchased Eugene-based Oregon Medical Group and Portland-based GreenField Health. Combined, the two systems have about 120 doctors and clinicians at 11 facilities.
GreenField Health was purchased last year and Oregon Medical Group in late 2020, according to the Lund Report.
Nationwide, UnitedHealth Group has purchased about 1,500 primary care and specialty facilities, totaling 60,000 physicians.
Humana will divest its majority stake in Kindred at Home’s hospice business to investment firm Clayton, Dubilier & Rice.
As part of the deal, which was announced Thursday, Humana will sell off a 60% stake in KAH Hospice for $2.8 billion in cash, which reflects an enterprise valuation of $3.4 billion and twelve times the division’s forecasted earnings before interest, income taxes, depreciation and amortization (EBITDA) for this year.
Humana said a year ago when it bought out the majority stake in Kindred at Home that it planned to divest the hospice arm. The insurer believes that it can deliver strong patient outcomes in hospice care without owning KAH Hospice outright, Chief Financial Officer Susan Diamond said in a statement.
Bay Area biotech Guardant Health is closer than ever to its ultimate goal — developing and deploying a simple, blood-based test that you could get during an annual doctor’s visit to spot cancer early enough that it might be treated more successfully. And 2022 is shaping up to be a big year for the company’s ambitions.
Today is Earth Day. AHRQ offers “A new AHRQ Views blog post in recognition of Earth Day 2022 highlights the Agency’s emerging efforts to reduce the impacts of climate change.”
From the FEHB front, Fedweek warns federal employees to think hard before rejecting FEHB coverage late in a career. As explained in the article you can lose out on one of the best fringe benefits for federal and postal employees — continuing their FEHB coverage into retirement with the full government contribution.
From the Omicron and siblings front —
STAT News informs us
Experts who advise the CDC met yesterday to discuss a thorny issue: Covid vaccine boosters, specifically the new policy to allow people 50 and older and people who are immunocompromised to get a second booster. By the end of the meeting — during which members of the Advisory Committee on Immunization Practices expressed frustration with the lack of clarity about the goal of the U.S. booster policy — it wasn’t entirely clear why people are being offered a second booster at this time. Data presented by CDC experts suggested the protection that immune-competent people have received from their primary series and first booster is holding up and the expected benefits from the fourth shots are modest at best. ACIP member Beth Bell raised concerns about “booster fatigue” and said offering another dose now could undercut confidence in vaccines that are working well at protecting people from severe Covid. The policy to offer the fourth doses was made without consulting ACIP.
What’s more,
Among the many views expressed around vaccine mandates, one theme persists: the idea that Covid-19 infection protects unvaccinated people against reinfection. While CDC says “getting a Covid-19 vaccination is a safer and more dependable way to build immunity to Covid-19 than getting sick with Covid-19,” a research letter in JAMA Network Open tested the concept of natural immunity by analyzing data from more than 121,000 patients receiving health care in the western U.S. from October 2020 through November 2021, before the Omicron variant took hold. Unvaccinated people who’d been sick with Covid had an 85% lower risk of acquiring Covid again compared to unvaccinated individuals without prior Covid. That level is similar to what mRNA vaccines deliver. Previous infection conferred 88% protection against hospitalization after reinfection and 83% protection against reinfection that did not require hospitalization. The authors conclude natural immunity works as well against both mild and severe illness. One difference: Natural immunity didn’t wane, but mRNA vaccines’ protection did. “This study may have important implications for vaccine policy and public health,” they write.
It is illogical to downplay natural immunity when the worst flu epidemic in U.S. history, the 2018 pandemic, was resolved by a combination of deaths and natural immunity. This is not intended to downplay vaccines. In the FEHBlog’s view, the CDC should be paying more attention to natural immunity from Covid.
From the Covid anti-fraud front, Healthcare Dive reports
The Department of Justice has charged 21 people across the U.S. for pandemic-related healthcare fraud, federal prosecutors said Wednesday.
Defendants — including doctors, medical business executives and fake vaccination card manufacturers — caused nearly $150 million in false billing to federal programs, the DOJ alleged.
The prosecution effort involves some of the “largest and most wide-ranging pandemic-related frauds detected to date,” said Kevin Chambers, the DOJ’s director for COVID-19 fraud enforcement.
From the Food and Drug Administration front —
The American Hospital Association tells us
The Food and Drug Administration seeks comments through June 21 on a potential change that would require outpatient settings to dispense opioid pain medications with prepaid mail-back envelopes and pharmacists to provide patient education on safe disposal of opioids.
“This potential modification to the existing Opioid Analgesic Risk Evaluation and Mitigation Strategy would provide a convenient, additional disposal option for patients beyond those already available such as flushing, commercially available in-home disposal products, collection kiosks and takeback events,” the agency said.
Good idea. Also
Health care providers should not use non-invasive prenatal screening tests alone to diagnose genetic abnormalities due to the potential for false results, the Food and Drug Administration warned last week. Also known as cell-free DNA tests or non-invasive prenatal tests, these laboratory developed tests in most cases are not reviewed by the FDA.
“Patients and health care providers should be aware of the risks and limitations of using these genetic prenatal screening tests and that they should not be used alone to diagnose chromosomal (genetic) abnormalities,” FDA said, citing reports that some patients and providers have made critical health care decisions based on the results without additional confirmatory testing.
Thanks to Covid-19 vaccines and therapies, U.S. spending on pharmaceuticals rose 12% in 2021 as use reached record levels and new prescriptions for acute and chronic care largely recovered from the slowdown seen during the pandemic, according to a new analysis.
Meanwhile, out-of-pocket costs paid by patients hit $79 billion, a $4 billion rise from the year before and the same level seen in 2018 after two years of declining costs. Overall, these costs were relatively low — less than $20 per prescription — but about 1% of all prescriptions filled, or 64 million, ran patients $125, underscoring ongoing barriers to affordability. In fact, 81 million prescriptions were not filled last year.
“We’re not in a very different situation from where we were five years ago except for the intensified, competitive market dynamics. But there are no major changes from a major legislative or policy perspective,” said Murray Aitken, senior vice president and executive director of the IQVIA Institute for Human Data Science, which conducted the analysis.
He also noted that the overall use of health services has returned to pre-pandemic levels, but has not yet made up for the backlog in missed patient visits, screenings and diagnostics, elective procedures, and new prescription starts — which IQVIA called a “concerning gap in preventive and treatment services.”
From the opioid epidemic front, the White House announced today
President Biden sent his Administration’s inaugural National Drug Control Strategy to Congress at a time when drug overdoses have taken a heartbreaking toll, claiming 106,854 lives in the most recent 12-month period. The Strategy delivers on the call to action in President Biden’s Unity Agenda through a whole-of-government approach to beat the overdose epidemic.
The Strategy focuses on two critical drivers of the epidemic: untreated addiction and drug trafficking. It instructs federal agencies to prioritize actions that will save lives, get people the care they need, go after drug traffickers’ profits, and make better use of data to guide all these efforts.
The Centers for Disease Control and Prevention on Wednesday asked the Justice Department to appeal a federal judge’s ruling overturning the federal mask mandate for airlines and other forms of public transportation, setting up a legal battle that could permanently impact the CDC’s ability to weigh in on public health issues.
The judge’s ruling was the latest in a series of court decisions that have left the Biden administration with dwindling legal options for mandates to combat Covid-19. And it came amid a shift away from mask mandates in the U.S., even in Democratic-controlled states along the East and West coasts. An appeal gives the Biden administration the opportunity to persuade a higher court to wipe the Florida ruling off the books, which could prove useful to the White House if it chooses to pursue a mask mandate in the future.
A new U.S. government center [residing within the CDC] aims to become the National Weather Service for infectious diseases — an early warning system to help guide the response to COVID-19 and future pandemics.
The new Center for Forecasting and Outbreak Analytics launched Tuesday. Its leaders say predicting the course of the COVID-19 pandemic in the U.S. has been hampered by data-collection problems.
In contrast, the United Kingdom uses regular population sampling with swab tests and blood draws to get a clearer picture of who’s been infected, said Marc Lipsitch, the new center’s science director. He said similar sampling should be considered in the U.S.
And the Centers for Disease Control and Prevention needs to have better access to data from state governments and hospitals, said Caitlin Rivers, the center’s associate director.
From the Omicron front, STAT News discusses six Covid mysteries that scientists are beginning to unravel.
Hospitalization rates for unvaccinated children ages 5 to 11 were twice as high as among those who were vaccinated during the record COVID-19 surge caused by the Omicron variant, according to a U.S. study released on Tuesday.
For every 100,000 unvaccinated children in the age group, 19.1 per were hospitalized with COVID-19 between mid-December and late February, compared with 9.2 per 100,000 vaccinated kids, the U.S. Centers for Disease Control and Prevention reported.
From the Social Determinants of Health front,
The Center for Medicare Services “outlined an action plan that demonstrates the Biden-Harris Administration’s ongoing efforts to provide high-quality, affordable health care for all people, regardless of their background, and to drive health equity across the Department of Health and Human Services (HHS).”
“The goals of CMS’ action plan include:
Promoting culturally and linguistically appropriate services in organizations;
Enrolling more people in Medicare, Medicaid, the Children’s Health Insurance Program and Health Insurance Marketplace; and
Incorporating screening for and promoting broader access to health-related social needs.”
The CDC’s Division of Diabetes Translation called attention to its new website on improving health equity
From the No Surprises Act front, the American Medical Association offers an article on how doctors can use the NSA to resolve billing disputes. It’s always helpful to take a peek at the other sides’s strategies.
Beginning in August, Kaiser Permanente commercial HMO and exclusive provider organization (EPO) members who need urgent care when they are traveling outside of areas served by Kaiser Permanente will have access to Cigna’s national PPO network of more than one million physicians and other providers. This will significantly expand Kaiser Permanente’s ability to provide more affordable and convenient access to valuable, high-quality health care and services for current and future members.
This is a smart move by KP to reduce its exposure to NSA emergency department billing disputes.
In the area of specialty pharmacy services, the agreement seeks to deliver overall value and savings to Kaiser Permanente and its commercial plan members. Accredo, Evernorth’s specialty pharmacy, will become Kaiser Permanente’s preferred external pharmacy for limited distribution drugs, and Evernorth’s CuraScript SD will be a preferred distributor for purchasing certain other specialty products.
The broad agreement between Evernorth and Kaiser Permanente is effective immediately.
Anthem’s first-quarter profits reached $1.8 billion thanks to strong enrollment in its Medicaid and Medicare Advantage plans.
Anthem, which operates an array of government and commercial health insurance including Blue Cross and Blue Shield plans in 14 states, Wednesday reported first-quarter profits rose 8.4% to $1.8 billion, or $7.39 per share, compared to $1.67 billion, or $6.71 per share, in the year-ago quarter. Revenue rose nearly 17.6% to $38 billion compared to $32,4 billion a year ago.
Anthem’s membership grew by 3.3 million, or 7.5%, to 46.8 million as of March 31, 2022, compared to a year ago.
According to the report, only 4.6% of hospitals were sold over the period. Small hospitals with 26-64 beds were more likely to be acquired than larger hospitals, and hospitals with the greatest negative margins were over twice as likely as those with the highest positive margins to be acquired (8.6% versus 3.0%). Only one critical access hospital was acquired during the study period, and urban hospitals were more likely to be acquired than rural hospitals (5.6% versus 3.3%). Long-term care hospitals were the most likely to be acquired, while psychiatric and “other” hospitals were the least likely.
The agency plans to update the data on a quarterly basis.
When comparing the use of telehealth among different pediatric subspecialties, a JAMA Network Open study found that pediatric telehealth use was inconsistent across subspecialties, with genetics and behavioral health subspecialists using the care modality the most.
The study included 549,306 patients, representing a total of 1.8 million visits from eight pediatric medical groups from the Children’s Specialty Care Coalition (CSCC). There were 11 different subspecialties, including cardiology, orthopedics, urology, nephrology, dermatology, genetics, behavioral health, pulmonology, endocrinology, gastroenterology, and neurology. The study period began Jan. 1, 2019, and ended Dec. 31, 2021.
The White House and the U.S. Department of Health and Human Services (HHS) are hosting an upcoming meeting entitled, Conversations on Encouraging COVID-19 Vaccinations, a virtual program that is part of the “We Can Do This” COVID-19 public education campaign.
The virtual Summit will feature conversations among leading doctors, medical professionals, parents, and community leaders about COVID-19 vaccines and how the broader medical community can encourage vaccination among pregnant people, children, teens, and young adults.
Speaking of AHIP, the FEHBlog noticed today that the OPM AHIP FEHB carrier conference website is fully built out. The virtual conference will be held on April 27 and 28.
The Biden administration Monday said it would not enforce the mask mandate for airplanes and transit after a federal judge in Florida struck it down.
In a 59-page order, U.S. District Judge Kathryn Kimball Mizelle said the Centers for Disease Control and Prevention overstepped its authority by requiring passengers to wear masks on public transportation, saying the mandate ”exceeds the CDC’s statutory authority and violates the procedures required for agency rulemaking.”
The Biden administration responded late Monday with a statement saying that the agencies are reviewing the decision and assessing possible next steps. * * *
The CDC recommended that people continue to wear masks in indoor public transportation settings.
United, American, Southwest, Delta and Alaska and other airlines late Monday said they were dropping their face mask requirement effective immediately given a federal judge’s ruling in Florida and the White House response to it.
From the Medicare front, the Centers for Medicare Services announced
a proposed rule for inpatient and long-term hospitals that builds on the Biden-Harris Administration’s key priorities to advance health equity and improve maternal health outcomes. In addition to annual policies that promote Medicare payment accuracy and hospital stability, the FY 2023 Inpatient Prospective Payment System (IPPS) and Long-Term Care Hospital (LTCH) Prospective Payment System (PPS) rule includes measures that will encourage hospitals to build health equity into their core functions, thereby improving care for people and communities who are disadvantaged and/or underserved by the healthcare system. The rule includes three health equity-focused measures in hospital quality programs, seeks stakeholder input related to documenting social determinants of health in inpatient claims data, and proposes a “Birthing-Friendly” hospital designation.
For acute care hospitals paid under the IPPS that successfully participate in the Hospital Inpatient Quality Reporting Program and are meaningful electronic health record users, the proposed increase in operating payment rates is projected to be 3.2%. This reflects a FY 2023 projected hospital market basket update of 3.1% reduced by a projected 0.4 percentage point productivity adjustment and increased by a 0.5 percentage point adjustment required by statute. Under the LTCH PPS, CMS expects payments to increase by approximately 0.8% or $25 million. * * *
The American Hospital Association’s statement on the proposed rule may be found here. The regulatory battle has been joined.
From the medical research front
Medpage Today offers access to “a video [in which], Scott Weiner, MD, MPH, director of the Brigham Comprehensive Opioid Response and Education (B-CORE) Program at Brigham and Women’s Hospital in Boston, discusses his recent study on the risks of chronic use and overdose with hydrocodone versus oxycodone and how providers can keep their patients safe when prescribing these medications.” A transcript of the video also is provided.
Higher levels of “good” cholesterol in the fluid surrounding your brain and spinal cord may help protect you from Alzheimer’s disease, a new study suggests.
“This study represents the first time that small HDL particles in the brain have been counted,” said study co-author Dr. Hussein Yassine. He is an associate professor of medicine and neurology at the University of Southern California’s Keck School of Medicine in Los Angeles.
For the study, Yassine and his colleagues analyzed concentrations of high-density lipoproteins (HDL) — often referred to as “good cholesterol” — in the cerebrospinal fluid of 180 healthy volunteers with an average age of nearly 77.
The study linked a higher number of small HDL particles in cerebrospinal fluid with two key indicators that they might protect against Alzheimer’s. * * *
The results suggest that small HDL particles may point the way to treatments for early Alzheimer’s, long before mental decline occurs.
The nation’s preeminent cancer hospitals are charging commercial health insurers anywhere from double to seven times their costs of acquiring cancer drugs, a new study shows.
Most top cancer institutions also are keeping their drug prices secret in direct violation of federal law, potentially exposing themselves to fines.
The findings reinforce how cancer care, especially the drugs, generates significant revenue for hospitals, and how markups on drugs potentially put insured cancer patients in financially perilous situations. * * *
Ultimately, researchers found the amount of money that a hospital gets from an insurance company, just for the cancer therapy, often is more than what the drug company receives.
So it’s not just insulin. No bueno.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.