
Weekend update
Congress is now in recess until after Labor Day. Here’s a link to last week’s news up on the Hill.
The New York Times had two stories that bear on our beloved FEHBP this weekend. The first concerned a claim dispute involving an FEHBP HMO where after about five years of going back and forth with a member about coverage of health care trial related expenses the carrier agreed to pay around $200,000 in benefits plus another $180,000 in interest calculated at the rate that the carrier charges when it is collecting overpayments from healthcare providers (18%). The ACA now generally requires plans to cover these expenses.
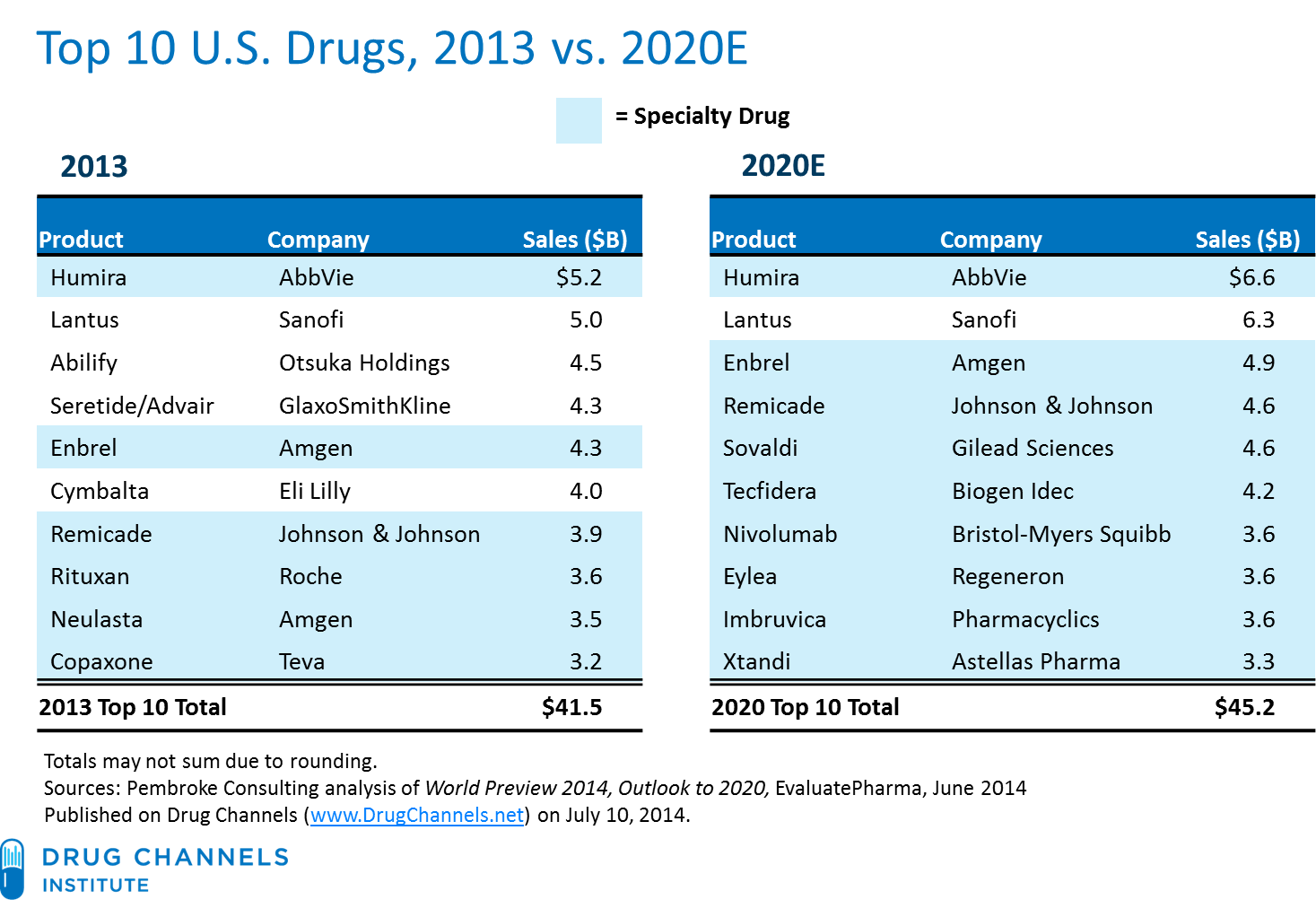
The other story reviews the controversy over Gilead Science’s pricing policy for its Sovaldi drug that treats Hepatitis C. Pricing is as much of an art as it is a science. In the FEHBlog’s view, Gilead deserves a lot of credit for developing this drug but it could not be charging $1,000 a pill with the price support provided by health insurers. Gildead’s $1,000 per pill price has raised the bar for all types of drugs where the market is constricted, e.g., vaccines. The article strikes a hopeful tone that the crisis will be shortlived. Hope does spring eternal.
Medcity News interviews the head of development at Cambia Health Solutions (Regence Blue Cross). The insurer certainly has its fingers in a lot of pies as part of its effort to control healthcare costs.
Many of its wholly owned companies grew out of internal projects. hubbub health is a company initially built for its health plan clients but which now extends to a broader customer base. Healthsparq, which uses price transparency to guide employer plans, was originally developed for its own plan customers but now serves 65 health plans. Other examples include Wellero, LifeMap, SpendWell and OmedaRx.
But Cambia investments span a much broader range of categories and include many technology-enabled services. There’s Wildflower Health, which is about high-risk pregnancy and pregnancy management, particularly for Medicaid patients; Qliance — a primary care provider; ClearCare — a health IT company for home healthcare agencies, Live!y — a remote monitoring sensor producer to support aging in place; CoPatient — a healthcare bill review service; Retrofit — a weight loss program using wireless devices and apps; and PockitDoc.
Interesting.

{kind=link}