Federal cyber officials will formally ask industry leaders “in the next couple of days” to help shape the regulatory structurefor cybersecurity incident reporting, Jen Easterly, director of the Department of Homeland Security’s Cybersecurity and Infrastructure Security Agency, said Wednesday.
The incident reporting framework follows the new law that President Biden signed in March requiring that critical infrastructure owners and operators to report major cyberattacks to CISA within 72 hours and ransomware attacks within 24 hours.
CISA has said that it will use the reports to rapidly deploy resources to victims under attack and share information with network defenders. Easterly, who spent four years working on cyber defense at Morgan Stanley prior to coming to CISA, emphasized that she wants to work with industry to create a smart regulatory apparatus that doesn’t create problems for the private sector.
“This will finally allow us a much better understanding what’s going on across the ecosystem,” Easterly said at the Billington Cybersecurity Summit in Washington. “We don’t want to burden industry and we don’t want to burden the federal government with noise either.”
Easterly said that after CISA issues a request for information from the private sector, she intends to also host several listening sessions with industry to ensure the rule-making process is “consultative.”
Healthcare data breaches are continuing to impact the healthcare sector at alarming rates, even as more organizations adopt updated security solutions in an attempt to keep pace with the influx of new cyber threats.
The healthcare sector suffered about 337 breaches in the first half of 2022 alone, according to Fortified Health Security’s mid-year report. More than 19 million records were implicated in healthcare data breaches in the first six months of the year.
What’s more, IBM’s annual “Cost of a Data Breach” report showed that the average cost of a healthcare data breach is now $10.1 million per incident, signifying a 9.4 percent increase from its 2021 report.
Nearly 90% of information technology professionals working in health care said their facilities suffered a cyberattack in the past year, according to a report out Thursday from the research organization Ponemon Institute.
Many of them said the attacks, which averaged 43 at various types of health care organizations including hospitals and insurance providers, increasingly affected patient care.
More than 600 IT and IT security practitioners responded to the survey sponsored by the cybersecurity firm Proofpoint. The report comes amid frequentwarnings from federal cybersecurity officials about ransomware and other cyberattacks on health care organizations.
Fifty-three percent of the respondents said their organization had experienced at least one ransomware incident over the past two years, while a third said they’d suffered between two and five. Nine percent of respondents said their organizations suffered six to 10 incidents.
The findings mark an increase from a year ago when Ponemon conducted a similar survey commissioned by cybersecurity firm Censinet. That survey found that just over 40% of respondents suffered a ransomware attack in the previous year.
Security Week adds “Security researchers with AT&T Alien Labs are warning of a new piece of malware that can take full control of infected Linux systems, including Internet of Things (IoT) devices. Dubbed Shikitega, the threat is delivered as part of a multi-stage infection chain, where each step is responsible for a part of the payload and fetches and executes the next module.”
Barely one in five organizations consider their organization as prepared as possible for a potential ransomware attack, according to a survey of 400 IT leaders and professionals involved in their company’s cybersecurity strategy. Almost 15% said they are very or somewhat unprepared for an attack.
The majority of respondents said they spend less than five hours per week on ransomware preparedness. Almost one-third invest less than an hour per week on the matter.
Organizations’ perceived state of preparedness and time spent bolstering defenses against ransomware stands out considering how many have already been hit. More than four out of 10 respondents said they’ve had a ransomware attack that resulted in infiltration or data encryption.
Here’s a link to the latest Bleeping Computer’s Week in Ransomware for your reading pleasure.
In cybersecurity leadership news —
Cybersecurity Dive discusses “Today’s top cybersecurity concerns and what comes next; CISOs are up against talent shortages and retention concerns amid an increasingly sophisticated threat landscape.
The Wall Street Journal reflects on “Why Companies Need to Think About Cyber Resilience, Not Just Cybersecurity; Cyber resilience concedes that breaches are inevitable, and it makes minimizing risk or loss in the event of an attack the end goal.”
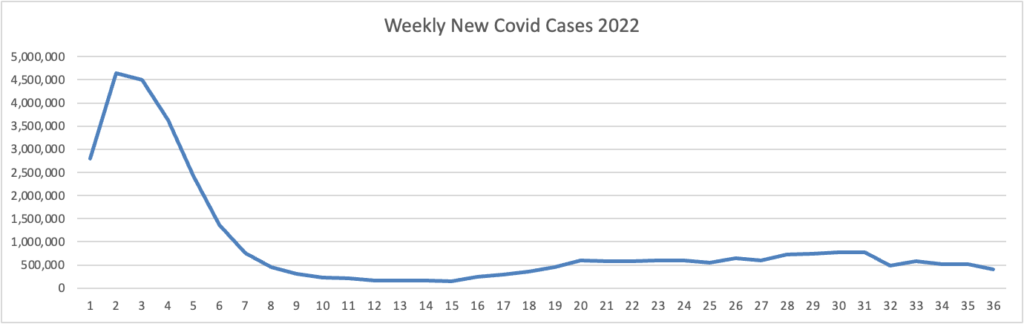
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first week, here is the FEHBlog’s updated weekly chart of new Covid cases for 2022:
The enormous surge on the right is the original Omicron strain. Its sibling variants follow. The CDC’s weekly review of its Covid stats is back this week:
As of September 7, 2022, the current 7-day moving average of daily new cases (70,488) decreased 18.8% compared with the previous 7-day moving average (86,853).
CDC Nowcast projections* for the week ending September 10, 2022, estimate that the combined national proportion of lineages designated as Omicron will continue to be 100% with the predominant Omicron lineage being BA.5, projected at 87.5% (95% PI 86.2-88.7%).
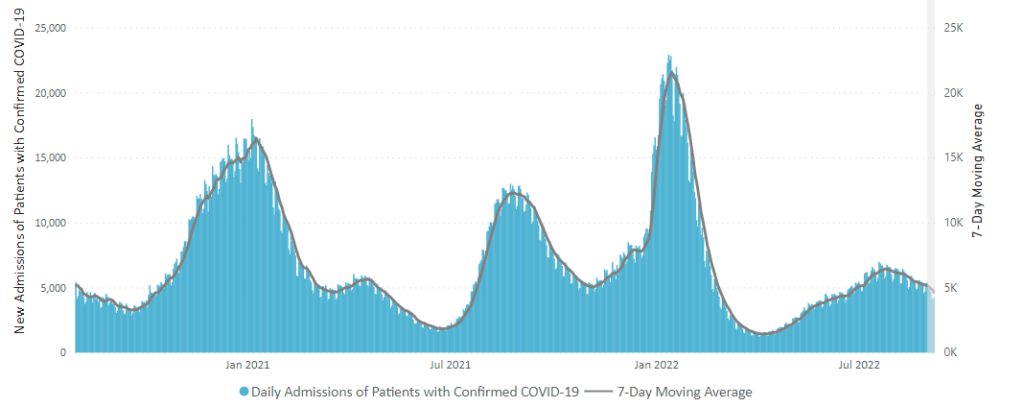
Here is the CDC’s current chart of daily trends of new Covid hospitalizations:
The CDC’s weekly review adds “The current 7-day daily average for August 31–September 6, 2022, was 4,620. This is a 10.5% decrease from the prior 7-day average (5,163) from August 24–30, 2022.”
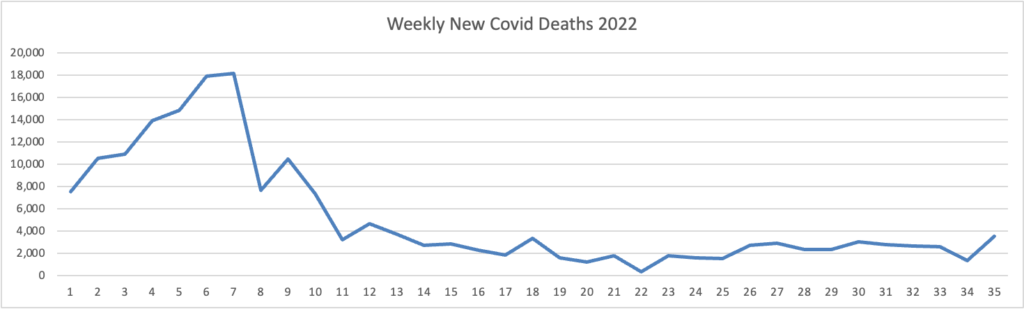
Here’s the FEHBlog’s weekly chart of new Covid deaths for 2022 which also is trending down.
The CDC’s weekly review adds “The current 7-day moving average of new deaths (314) has decreased 28.1% compared with the previous 7-day moving average (437).”
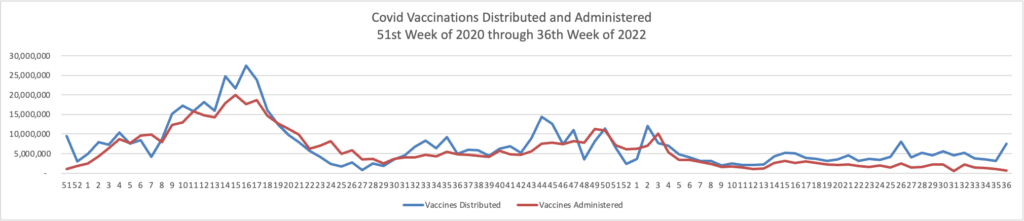
Here’s the FEHBlog’s chart of Covid vaccinations distributed and administered from the beginning of the Covid vaccination era (51st week of 2020) through the 36th week of 2022.
As of September 7, 2022, 610.7 million vaccine doses have been administered in the United States. Overall, about 263.1 million people, or 79.2% of the total U.S. population, have received at least one dose of vaccine. About 224.4 million people, or 67.6% of the total U.S. population, have been fully vaccinated.*
Of those fully vaccinated, about 109.0 million people have received a booster dose,* but 50.0% of the total booster-eligible population has not yet received a booster dose. Booster dose eligibility varies by age and health condition. Learn more about who is eligible.
Last week, according to the CDC’s stat review, the CDC’s Covid community level evaluations saw an 8.6% decrease in high-level communities and a 10.2% increase in low-level communities.
In other Covid news, Benefits Pro discusses a Brookings Institution report on long Covid’s impact of the U.S. workforce, and the Society for Human Resource Management offers an article confirming the FEHBlog’s take on the recent federal appellate court decision concerning the federal government’s stayed vaccine mandate on federal government contractors.
A federal judge grilled the Justice Department on Thursday over its antitrust claims that UnitedHealth Group Inc.’s $13 billion acquisition of health-technology firm Change Healthcare Inc. would suppress competition and limit innovation in health insurance markets.
During closing arguments, U.S. District Judge Carl J. Nichols questioned the department’s arguments that he should block the deal because it would limit competition for technology used in claims processing and would give UnitedHealth access to sensitive industry data that it could use to harm competitors. * * *
Judge Nichols is expected to issue his ruling in the coming weeks.
Home improvement retailer Home Depot and two other, smaller employers are appealing a recent $2.67 billion settlement that covers allegedly anticompetitive behavior from Blue Cross Blue Shield insurers.
The appeals could potentially delay the release of the funds and the broader terms of the settlement, which U.S. District Judge R. David Proctor finalized in August.
Negotiations are intensifying over massive, multibillion-dollar legislation to fund the Food and Drug Administration, with just weeks left before the current agreement expires, four sources following the talks said. * * *
Talks are still fluid, and there is no final agreement yet. Lawmakers are aiming to finalize a package by early next week.
The FDA agreement could ride along with a government funding package before the end of September, when government funding runs out. There’s a chance the user fee legislation could pass on its own, however, if there is a bipartisan deal. The Democrats’ user fee offer was a full five-year agreement, not a shorter-term deal.
From the fraud, waste, and abuse front, Beckers Hospital Review informs us
A small number of primary care providers have been responsible for most of the recent growth in remote patient monitoring, though it’s not known how much their patients needed that type of potentially expensive care, a new Health Affairsstudy found.
Remote patient monitoring grew fourfold during the pandemic’s first year, according to the analysis of OptumLabs Data Warehouse data from January 1, 2019, to March 31, 2021. The database includes Medicare Advantage claims that total about 20 million people annually.
Out of a group of 342 high-volume providers, 0.1 percent accounted for 69 percent of all general remote patient monitoring claims, the Sept. 6 study found.
But the Harvard University researchers said they didn’t observe that the high-volume providers targeted patients with more severe or uncontrolled disease. They said growth rates “indicate that total spending on remote patient monitoring could quickly escalate” and potentially burden CMS and other payers financially.
“More research is needed to identify which patients and use cases benefit most from remote patient monitoring,” the study’s authors wrote. “In the meantime, payers and policymakers should closely monitor its use and be prepared to establish appropriate controls as informed by new evidence.”
From the mental healthcare front, the American Hospital Association relates
The Department of Health and Human Services today reported a 45% increase in call volume and improved answer rates and wait times for the 988 Suicide and Crisis Lifeline this August compared to a year ago. The 10-digit National Suicide Prevention Lifeline in July transitioned to the 988 Suicide and Crisis Lifeline, meaning individuals experiencing a suicide, mental health or substance use crisis can simply call, chat or text 988 to connect with a trained crisis counselor.
The Substance Abuse and Mental Health Services Administration also announced a $35 million grant opportunity to better support 988 Lifeline services in tribal communities, which face unique challenges to accessing technology and crisis services.
Republican lawmakers are pushing back on the Biden administration’s request for an additional $26 billion in COVID-19 and monkeypox funding, the AP, Politico and other news sources reported.
The White House’s ask came as Congress begins negotiations for a short-term funding bill needed to avoid a shutdown at the end of the month.
In comments to reporters, conservatives said their disapproval of additional pandemic spending was tied to inflation and concerns about how prior funds were used.
“The problem is they want to keep spending more money and throw more gasoline on the inflation fire,” Senator John Cornyn (R-Texas) told the AP. “I think that’s a bad idea.”
The lawmakers said that the White House should instead repurpose funds left over from earlier pandemic asks and begin transitioning the costs for certain efforts, such as vaccines, to the private sector or general public.
“There’s really no reason that the government should be paying for all of that,” Senator Roy Blunt (R-Mo) told the AP.
Infectious disease specialists [writing in a recent New England Journal of Medicine report] say the rebounds aren’t uncommon, and patients should watch for them. They should also feel reassured that symptoms are almost always mild when a rebound occurs.
Because a rebounder can become contagious again, the Centers for Disease and Control and Prevention urges people to re-isolate and mask if symptoms recur and rapid tests turn positive again.
Specialists emphasize that though rebounds are an inconvenience, Paxlovid remains the treatment of choice for people at high risk of severe Covid.
Politico reports that doctors and Reuters reports that researchers are colloborating to understand and treat long Covid.
As the FEHBlog received his bivalent mRNA booster yesterday, it’s worth pointing out this advice from STAT News
If you’re planning to double up your new Covid booster with your annual flu shot in one visit this month, you might want to reconsider. Even though White House Covid coordinator Ashish Jha believes “this is why God gave us two arms — one for the flu shot and the other one for the Covid shot,” it’s still early to get a flu shot, STAT’s Helen Branswell warns. That’s because protection generated by flu vaccines erodes pretty quickly over the course of a flu season.
A flu vaccine dose given in early September may offer limited protection if the flu season doesn’t peak until February or even March, as it did during the unusually late 2021-2022 season. “You’ve got about four months of pretty solid protection,” Emily Martin, an epidemiologist who specializes in flu at the University of Michigan School of Public Health, told Helen. Read what other experts had to say.
* Demetre Daskalakis, a White House health official, said the monkeypox outbreak has slowed significantly since July as vaccination efforts have ramped up.
* The U.S. is still battling the largest monkeypox outbreak in the world with nearly 21,000 cases reported across all 50 states, Washington D.C. and Puerto Rico, according to CDC.
* The U.S. has administered more than 460,000 monkeypox vaccine doses so far, according to data from 35 states.
From the healthcare costs front, Health Payer Intelligence reports
Almost 83 cents of the average healthcare premium dollar goes towards prescription drugs and medical services, including inpatient and outpatient costs, emergency room costs, and doctor visits, according to research from AHIP.
AHIP analyzed data from commercial health insurance plans between 2018 and 2020 to determine how payers spend member premiums. The research reflects spending by employer-sponsored health plans and health plans in the individual market.
“This 3-year trend data includes the first year of the COVID-19 pandemic, when healthcare utilization was down dramatically as patients deferred care and isolated due to the risk of infection,” Matt Eyles, president and chief executive officer of AHIP, said in a press release.
Prescription drugs accounted for the largest portion of the premium dollar at 22.2 cents—up from 21.5 cents between 2016 and 2018. Prescription drug expenses include payments for outpatient prescription medications obtained from the pharmacy or medicines administered in a physician’s office or clinic.
The next largest chunk of the healthcare dollar (19.9 cents) went toward outpatient hospital costs. This includes physician and facility payments for treatment in the outpatient department of hospitals, such as receiving an X-ray or seeing a primary care physician. However, it does not include emergency room costs, such as payments for emergency room visits and ambulance transportation, which accounted for 3.3 cents of the premium dollar.
Inpatient costs represented 19 cents of the dollar, AHIP found. These expenses include payments for all services during hospitalization, including payments to physicians, facility payments, costs for prescription drug administration, and room and board costs.
Almost 12 cents per dollar went toward doctor visits, which included payments to physicians for services provided in an office, clinic, or urgent care facility. The 11.8 cents also went toward equipment and supplies used during a visit and nursing staff salaries.
playbook, “Beyond Hospital Transparency: Getting to Fair Price,” helps purchasers navigate and understand how to best leverage newly available hospital price and quality transparency data and tools from Sage Transparency which incorporates content from RAND Corporation, the National Academy for State Health Policy (NASHP), and other sources. It also offers guidance on rights and responsibilities as plan sponsor fiduciaries to determine fair prices for hospital services, market- and policy-based strategies, and ways to work individually and through coalitions to achieve fair pricing for hospital services.
While there isn’t a one-size-fits-all approach as available data and market conditions vary among regions and states, the methodology and action steps in the playbook to help plan sponsors determine and achieve a fair price include:
Identify breakeven costs – Uncover what hospitals need to charge commercial customers to break even considering all other incomes and expenses plus a reasonable margin.
Compare costs among peer hospital systems – Determine how hospital charges compare to other hospitals with similar services and quality.
Determine a fair market price – Use data from Sage Transparency to negotiate fees based on a reasonable markup of hospital costs.
OPM announced today that the next Federal Benefits Open Season will be held from November 14 through December 12, 2022. The announcement tells us that OPM expects to post 2023 FEHB and FEDVIP premiums on its website in “late September.”
From the Omicron and siblings front, the Wall Street Journal offers a helpful set of FAQs on the new bivalent mRNA boosters that are currently rolling out for administration.
From the monkeypox front, the Food and Drug Administration announced action to expand testing for the disease.
From the public health front, McKinsey and Company released its
United States of Health Dashboard. [McKinsey describes the tool as] an easy-to-use data visualization tool that enables users to explore the impact of disease and ill health within individual states, the dashboard is informed by key metrics encompassing maternal and neonatal health, behavioral health, communicable disease, chronic disease, and environmental health. It measures the total loss of healthy years of life, assuming full health (also known as “the burden of disease”), that affect a state’s population over the course of one year.
The dashboard is designed to help current and newly tapped state leaders, public-health agencies, and other stakeholders identify the highest-priority areas for investment by offering insights into key questions such as: How do behavioral health challenges affect a state’s population? How well is chronic disease managed and infectious disease controlled? How do mothers and their newborn infants fare? How well are health risks in the environment managed? And which populations are most significantly impacted by these metrics?
For example, here is a link to the Texas dashboard.
In other public health news, the American Hospital Association informs us
September is Suicide Prevention Awareness Month, with National Suicide Prevention Week running Sept. 4-10. In recognition of the effort to reduce the occurrence of suicide and destigmatize the conversation around it, AHA is proud to highlight resources available to our members and the public at large.
HR Director offers an interesting article about how HR professionals can approach this issue.
In the roughly dozen years since [he dealth with an employee suicide], [Matthew] Burr has advised every one of his clients (which include schools, financial firms and manufacturers, among other companies) to establish an EAP. Aside from a couple smaller companies, which have anywhere from five to 10 employees, every client has taken his advice. They were truly grateful to have done so ahead of the COVID-19 pandemic, so their employees had support systems already in place during the unprecedented time.
From the U.S. healthcare business front
Healthcare Dive reports that Walmart and UnitedHealthcare have teamed up to offer a Medicare Advantage plan under a ten-year-long contract. “Ultimately, the goal is to serve hundreds of thousands of seniors and Medicare beneficiaries in value-based arrangements through multiple Medicare Advantage plans.
Beckers Hospital Review tells us “Cost Plus Drug Co. founder Mark Cuban expects his online pharmacy to soon grow past 1 million customers, the billionaire of Shark Tank fame said Sept. 6 during Vox‘s Code Conference. ‘By the time I get back, we should, hopefully, be past a million patients in seven months,’ Mr. Cuban told Vox‘s Recode, referring to the late-January launch of Cost Plus Drug Co., according to CNET.”
Reuters reports, not surprisingly, that “CVS Health Corp’s (CVS.N) plan to buy healthcare services company Signify Health for about $8 billion will face a tough U.S. antitrust review even though the two companies do not compete directly in any markets, three experts said Tuesday.”
From the Rx coverage, BioPharma Dive discusses the near term future of biosimilar drugs.
From the health savings account front, Voya Financial discusses “five HSA funding strategies companies [or FEHB plans’ can employ to help boost employee saving.”
From Capitol Hill, Fierce Healthcare points out four legislative items that providers should be tracking for the remainder of this year.
From the Omicron and siblings front, the Washington Post reports
Cold weather favors the coronavirus. But as summer gives way to fall, infectious-disease experts are guardedly optimistic that the spread of covid-19 this autumn and winter won’t be as brutal as in the previous two years of the pandemic.
Coronavirus scenarios from multiple research teams, shared in recent weeks with federal officials, foresee stable or declining hospitalizations in early fall.The scenarios show the possibility of a late-fall surge. A new variant remains the biggest wild card. But several factors — including the approval this week of reformulated boosters and the buildup of immunity against the latest strain of the virus — could suppress some of the cold-season spread, experts say.
In related news, the Wall Street Journal informs us
U.S. health authorities plan to recommend that people get Covid-19 boosters once a year, starting with the new shots now rolling out, a shift from their current practice of issuing new advice every several months.
The annual cadence would be similar to that of flu shots, White House officials said Tuesday, though elderly people and those with weakened immune systems may need more frequent inoculations.
A shift to annual Covid-19 boosters would be a departure from current practice and comes after many people in the U.S. have ignored calls to get a first or second booster, partly due to fatigue with repeat inoculations.
“Barring any new variant curveball,” said White House coronavirus coordinator Ashish Jha, “for a large majority of Americans, we are moving to a point where a single annual Covid shot should provide a high degree of protection all year.”
A very sensible approach, indeed!
From the healthcare business front, Healthcare Dive tells us
Amazon and One Medical said Friday that antitrust regulators want more information about the online retailer’s proposed $3.9 billion acquisition of the primary care group.
The Federal Trade Commission sent a second request for information on Friday, One Medical said in a filing with the U.S. Securities and Exchange Commission.
A second request from the FTC means the two cannot move forward with the deal “until the companies have substantially complied with the additional investigatory request,” according to the FTC.
Amazon and One Medical will “promptly respond” to the second request, the primary care group said in the SEC filing.
Drug Channels surveys the upcoming Humira price war as biosimilar competitors take the field.
CMS posted new information about available group health plan defenses to CMS contractor assertions that the GHP has failed to properly coordinate its benefits with Medicare.
Beckers Payer Issues offers expert opinions on the impact of the transparency in coverage rule on consumerism now that the three machine-readable files of health plan pricing data have been posted for two months. For example, “Neil Mayle is the founder and president of Visible Charges, a Cambridge, Mass.-based company that provides clients with curated datasets of both payer- and provider-negotiated service prices. * * * ‘I think we’ve gone from nothing to a lot,’ Mr. Mayle said. ‘We haven’t gone to perfect.'” Of course, it was only the first of three stages in transparency in coverage rule disclosures.
The FEHBlog noticed today these CMS and DOL fact sheets on the No Surprises Act which are worth a gander.
The Senate returns to Capitol Hill for committee business and floor voting tomorrow. The Wall Street Journal adds “Between now and Election Day, senators are scheduled to be back in Washington for four weeks, then gone a week, and then back for two weeks in October.” The House of Representatives will be engaged in committee business but not floor voting this week. The House resumes floor voting next week.
The White House is asking Congress for $47.1 billion in emergency funding for Covid-19 and monkeypox and to back Ukraine in its war with Russia, as well as spending for natural disasters, according to administration officials.
Congress must vote on a spending bill by the end of September to avoid a partial government shutdown. Lawmakers are expected to use a stopgap funding measure that will maintain funding levels for the short term.
The White House is asking Congress to add the emergency funding on top of that, with about $22.4 billion for Covid-19 vaccines, testing programs, clinical trials and research; $4.5 billion to bolster efforts to fight monkeypox; and $6.5 billion to help areas of the country prepare for and recover from natural disasters. * * *
The emergency funds wouldn’t be paid for with new or shifted revenue, and would be new money that hasn’t been previously appropriated.
[As of last Friday, September 2] Senate Republican leadership didn’t immediately respond to a request for comment about the White House’s request for emergency funding. Spending bills require 60 votes, and in the 50-50 Senate at least 10 Republicans would need to back any bill that contained the administration’s request.
[President] Biden intends to nominate Richard Revesz, the AnBryce Professor of Law and Dean Emeritus at the New York University School of Law, to be administrator of the Office of Information and Regulatory Affairs, which is housed within the White House Office of Management and Budget. Biden has not had a permanent OIRA head since taking office.
From the U.S. healthcare business front, the Wall Street Journal reports this afternoon that CVS Health has struck a deal to purchase Signify Health:
The drugstore giant’s deal to acquire home-healthcare company Signify Health Inc., announced Monday, will add 10,000 contracted doctors and clinicians and give CVS a hand in coordinating medical care for millions of Americans.
CVS, the nation’s biggest healthcare company by revenue, said that it agreed to acquire Signify for $30.50 per share in an all-cash deal, confirming earlier Wall Street Journal reports. CVS said it expects the deal, finalized over the weekend after a sales process that drew interest from companies from Amazon.com Inc. to UnitedHealth Group Inc., to close in the first half of 2023.
CVS for years has worked to transform itself from a pharmacy chain to an integrated provider of medical services, with the biggest step being its 2018 acquisition of insurer Aetna. Initially, CVS envisioned a model centered on pharmacists, in-store clinics and a giant insurance business.
But Karen Lynch, who took over as CVS CEO last year, determined that the company needs doctors on its payroll to fulfill those ambitions. She also set out to expand CVS’s presence in home healthcare, demand for which has been rising as the U.S. population has aged.
Signify’s model is based on an analytics-and-technology platform, used by doctors that go into homes equipped with connected iPads, that allows the clinicians to assess patient needs and connect them with follow-up services.
The clinicians “operate much like Uber drivers,” said Kyle Armbrester, Signify Health chief executive. “We’re in a gig economy and this is a flexible model.”
The deal is the latest for a home-health company. Rival Walgreens Boots Alliance Inc. last week finalized a deal to purchase a majority stake in CareCentrix, Inc., another home-healthcare platform.
This spring, UnitedHealth agreed to buy LHC Group Inc., one of the country’s largest home-health firms, for about $5.4 billion. Last year, Humana Inc. agreed to take full control of home-health provider Kindred at Home. Both LHC and Kindred provide continuous home-healthcare services.
Signify has grown to serving more than 2.5 million homes from around 300,000 five years ago, said Mr. Armbrester, who is set to remain CEO of Signify Health after the acquisition.
From the public health front, NPR Shots discusses the new Covid boosters and Precision Vaccinations discusses flu shots. The FEHBlog checked chain pharmacies in his locality in Dripping Springs, TX. Flu shots are already available, and the new Covid boosters will be available mid-week.
The Health Sector Cybersecurity Coordination Center (HC3) issued a threat profile about Evil Corp and warned that the prolific group could threaten healthcare cybersecurity.
The Russian-based cybercriminal syndicate has been operational since 2009 and is responsible for creating some of the most powerful ransomware and malware variants. The group maintains strong connections to the Russian government and other cybercriminal gangs.
HC3 described the group as “exceptionally aggressive and capable.” Considering the group’s past crimes, this description seems highly accurate. In 2019, Evil Corp used Dridex malware to harvest login credentials from hundreds of banks, raking in more than $100 million in stolen funds.
Evil Corp should be considered a significant threat to the U.S. health sector based on several factors. Ransomware is one of their primary modus operandis as they have developed and maintained many strains. Many ransomware operators have found the health sector to be an enticing target as, due to the nature of their operations, they are likely to pay some form of ransom to restor operations. Healthcare organizations are particularly suceptible to data theft as personal health information (PHI) is often sold on the dark web to those looking to leverage it for fraudulent purposes. Foreign governments often find it to be more cost effective to steal research and intelliectual property via data exfiltration cyberattacks rather than invest time and money into conducting research themselves. This includes intellectual property related to the health sector. It is entirely plausable that Evil Corp could be tasked with acquiring intellectual property from the U.S. health sector using such means at the behest of the Russian government.
Bleeping Computer, which is not offering the Week in Ransomware this holiday weekend, delves into the Lockbit ransomware gang.
A critical, but long-anticipated decision by Lloyd’s last week to phase out coverage for state-sponsored cyberattacks illustrates an insurance market that has been under increasing financial pressure for years. It also raises questions for U.S. companies about their preparedness and long-term risks amid more dangerous and sophisticated threats.
“Cyber remains a priority area for Lloyd’s,” a spokesman said in an emailed statement. This month’s advisory guidance, “following consultation with our market, is to ensure we take on the right kinds of risk as a market while approaching this complex field with the expertise and diligence it requires.”
The company said it will continue to take a pragmatic and innovative approach to supporting the growth of cyber.
Lloyd’s policy says the company’s role is to support a competitive and resilient cyber insurance market, but the bulletin has not mandated clauses for managing agents. Instead of applying a one-size-fits-all approach, the new guidance encourages managing agents to apply due diligence to the specific complexities of state-sponsored attacks.
From the cyber defenses front —
Cybersecurity Dive discusses best practices for getting full value out of multi-factor authentication and a city for a passwordless future.
Health IT Security says, “When properly implemented, zero trust security strategies can help healthcare organizations bolster their security efforts. However, the sector faces unique challenges surrounding IoT devices and identity and access management that are worth considering when contemplating zero trust in healthcare. In a new white paper, Health-ISAC provided guidance for healthcare CISOs to help them understand and implement zero trust security strategies.”
ZDNet offers Microsoft guidance on how to reduce exposure to ransomware attacks.
CISA calls attention to necessary updates to certain Apple products.
Fortune lists “five free online cybersecurity courses hosted by top universities.”
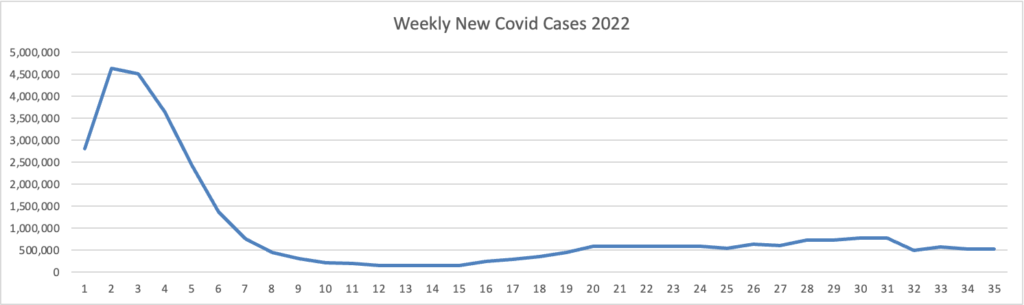
Because it’s the beginning of the three day weekend, the Centers for Disease Control did not publish its weekly review of CDC Covid statistics. The FEHBlog values that weekly review because it complements the FEHBlog’s own Covid charts which are based on the CDC’s Covid Data Tracker and use Thursday as the first day of the week. So without further ado, here are the FEHBlog’s three Covid charts for this week, the 35th week of 2022:
It’s always worth noting that the peaks on the left sides of the top two charts reflect the grand daddy of surges, the first Omicron wave. With respect to Covid vaccines, Revcycle Intelligence reports that the American Medical Association has added eight new CPT-4 codes to its procedures manual to cover physician services for the new Covid bivalent boosters.
From the U.S. healthcare business front, the Wall Street Journal reports this evening
CVS Health Corp. is in advanced talks to acquire the home-healthcare company Signify Health Inc. for around $8 billion, according to people familiar with the matter.
CVS appears to have beat out other heavy hitters including Amazon.com Inc. and UnitedHealth Group Inc., which had been circling Signify for a deal that could be announced soon. UnitedHealth never submitted an official bid, one of the people said.
There is still no guarantee that CVS will reach a deal for Signify, which has been exploring strategic alternatives since earlier this summer.
While Signify’s deadline for bids is Tuesday, September 6, Signify could strike a deal before then.
UHC is not sitting on its hands though. According to MedPage Today
UnitedHealth Group’s healthcare services division, Optum, will reportedly acquire Kelsey-Seybold for approximately $2 billion, according to the Star Tribune.
The acquisition of Kelsey-Seybold, a physician group based in Houston that includes cancer and women’s health centers, two ambulatory surgery centers, and a sleep center, was first announced in April, but few details have emerged since, the Star Tribunereported.
However, Optum, based in Eden Prairie, Minnesota, did provide a statement to MedPage Today about incorporating Kelsey-Seybold’s operations and staff into the Optum network.
From the rather quiet monkeypox front, STAT News raises a new concern.
A new study is raising concerns about the effectiveness of the monkeypox vaccine being used in the United States and other parts of the world.
The work, which has not yet been peer-reviewed, found that two doses of the vaccine induced relatively low levels of neutralizing antibodies against the monkeypox virus, and those antibodies had poor neutralizing capacity.
The researchers noted the so-called correlates of protection — what is needed, in terms of immune system weaponry, to be protected against monkeypox — are not known. Still, the evidence of low levels of neutralizing antibodies raises questions about how much protection is generated by two doses of the vaccine, marketed as Jynneos in the U.S. and made by the Danish manufacturer Bavarian Nordic. * * *
The study also casts a shadow over the recent decision by the U.S. government and others to stretch vaccine supplies by giving people one-fifth of a regular dose — and to do so by intradermal (into the skin) rather than subcutaneous (under the skin) injection. Intradermal administration, which requires smaller doses to be protective, has been shown to be effective in other disease outbreaks with other types of vaccine.
From the opioid epidemic front, STAT News features an interview with Rahul Gupta, M.D., “the director of the White House Office of National Drug Control Policy and the first doctor to hold that position.”
Gupta’s selection as director of the White House Office of National Drug Control Policy, however, has ushered in a new era of federal drug policy. As the first doctor to hold the position, he says he will embrace new strategies, including harm reduction tactics, which aim to reduce drug users’ risk of overdose, death, and disease in lieu of a hardline, abstinence-only attitude.
Still, though, addiction treatment is dogged by stigma, underuse of existing medications, and ongoing debate about certain harm-reduction techniques. The debate came to a head last week in California, where Gov. Gavin Newsom vetoed a bill to allow supervised injection sites — essentially clinics where people can use illicit drugs under medical supervision so as to prevent overdose.
Gupta sat down with STAT this week to discuss the ongoing crisis and the Biden administration’s efforts to address it. While circumspect about Newsom’s decision, Gupta did take several positions that are far more aggressive than any of his predecessors: Calling out doctors for their role in poor treatment outcomes; arguing that the addiction medication buprenorphine is widely misunderstood; and advocating for contingency management, a new addiction intervention that offers rewards — often cash — in exchange for cessation of drug use.
From the public health front, the Food and Drug Administrations discusses “Using A Whole-Of-Governments Approach to Combating Illicit Health Products.” Among other steps, “the agency has partnered with the Organisation of Economic Co-Operation and Development (OECD) Task Force on Countering Illicit Trade, which has been studying the problem of illicit trade for 15 years.”
From the Rx coverage front, Endpoints News informs us
Last July, the cost-effectiveness drug watchdog ICER released a preliminary draft report that Vivus’ Qsymia was the most cost-effective option for weight loss. That decision has now been validated.
ICER made its final determination Wednesday [August 31] that Qsymia, the brand name for the appetite suppressant phentermine combined with anticonvulsant topiramate, was more cost-effective for weight loss than other competitors such as Novo Nordisk’s Saxenda (liraglutide) and Wegovy (semaglutide) or Currax Pharmaceuticals’ Contrave (bupropion/naltrexone). * * *
ICER reviewers also added that if Qsymia wasn’t performing well in certain patients, Contrave may be the next best cost-effective option. The reviewers noted in their report that there were a few limitations to analysis, including the full impact of the drugs in patients with chronic kidney diseases or conditions where weight loss may be beneficial.
From the omicron and siblings front, AHIP informs us
Today the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP) voted to recommend the use of the bivalent mRNA COVID-19 vaccines as a single-dose booster for all individuals ages 12 and older (Pfizer-BioNTech) and 18 and older (Moderna), at least two months following primary series or previous booster dose. The ACIP recommendation for the bivalent boosters was approved by a vote of 13-1.
The Committee reviewed modeling data showing the vaccine has the potential to reduce hospitalizations and deaths, especially among high-risk groups. The bivalent boosters are recommended for all those over age 12 who have completed a primary series, at least 2 months after the most recent dose. The modeling data indicates that the vaccine is safe and effective, and that booster strategies will be executed in an equitable manner. Models also indicate that waiting until more trial data is available (in two to three months) could lead to preventable hospitalizations and deaths.
ACIP members expressed concern that many assumptions had been made with the modeling, and that the vaccine being recommended – which includes protections specific to the BA.4/BA.5 variants – has not been tested in humans. Mouse models were used for data on this vaccine, in addition to extrapolations from human trials using the BA.1-specific vaccine. CDC pointed out that annual influenza vaccines are modified based on projected variants without direct clinical evidence. ACIP members also expressed concerns that the bivalent booster makes assumptions about future variants, which this booster may not protect against.
Earlier this week, the Food and Drug Administration (FDA) amended the Emergency Use Authorizations (EUAs) for both the Moderna COVID-19 vaccine and the Pfizer-BioNTech COVID-19 vaccine to authorize bivalent formulations of the vaccines for use as a single booster dose at least two months following primary or booster vaccination. The bivalent Moderna vaccine is authorized for use as a single booster dose in individuals 18 years of age and older and the Pfizer bivalent vaccine is authorized for use as a single booster dose in individuals 12 years of age and older. FDA also released fact sheets on both the Pfizer-BioNTech vaccine and the Moderna vaccine.
With the authorization, FDA has revised the EUAs to remove the use of the monovalent versions of the vaccines for booster administration for the age groups now covered by the bivalent booster products. ACIP also rescinded its recommendations for the monovalent booster vaccines.
Bivalent boosters may be available as early as next week.
The FEHBlog finds it noteworthy that the new bivalent booster replaces the monovalent booster.
STAT News also discusses the Omicron outlook for this autumn.
In a way, some physicians have said, Covid is becoming more like the other respiratory pathogens that most of us shake off but that can occasionally cause severe illness and death among the oldest adults or people who are already sick. So many more people are dying from Covid than from those other viruses, however, because of the massive number of cases that are still occurring overall.
Another trend that has continued into 2022 has been the racial and ethnic disparities associated with Covid. The gaps between different demographic groups’ death rates have shrunk over time, but at the peak of this summer’s wave, for example, death rates by age group among Hispanic adults were notably higher than those among white adults, federal data indicate.
One of the silver linings of the pandemic is that, unlike with some viruses, SARS-2 did not pose a particularly serious threat to children. That’s not to minimize the hospitalizations and deaths — as well as incidents of long Covid and MIS-C — that the virus did cause in pediatric populations. But overall, kids have faced much lower risks of severe outcomes from Covid than adults.
Still, something worrisome occurred this summer with kids and Covid, as hospitalizations reached their second highest peak of the entire pandemic, surpassing last summer’s Delta wave and only trailing the initial Omicron spike early this year.
The article’s experts encourage vaccinating children to stem this tide.
From the FEHB front, Govexec provides a handy just before and just after federal retirement checklist, and Fedweek helpfully delves into “What Counts and What Doesn’t for Keeping FEHB Coverage in Retirement,” which should be a key consideration for career feds.
From the public health front, the CDC reminds us September is Sepsis Awareness Month
Anyone can get an infection, and almost any infection, including COVID-19, can lead to sepsis. Sepsis is the body’s extreme response to an infection and is a life-threatening medical emergency.
September is Sepsis Awareness Month and CDC encourages patients and healthcare professionals to share Get Ahead of Sepsis resources, below, to learn how to protect themselves, their loved ones, and their patients from sepsis:
Patients and families: * New this year is an updated patient and family brochure. * Download and share any of CDC’s FREE patient education materials with your friends and loved ones to learn how to prevent infections, be alert to the signs and symptoms of sepsis, and act fast if sepsis is suspected. * Share updated sepsis graphics on social media to educate friends and loved ones about sepsis. * Are your children back to school? Talk to your child’s healthcare professional and school nurse about steps you can take to prevent infections that can lead to sepsis. Some steps include taking good care of chronic conditions and getting recommended vaccines. Healthcare professionals: New this year are two fact sheets for long-term care nurses and certified nurse assistants. Download and share CDC’s FREE healthcare professional education materials with your colleagues to educate them about how to recognize signs and symptoms of worsening infection and sepsis, how to get ahead of sepsis, and what to do if they suspect sepsis. Educate your patients and their families about: o Preventing infections o Keeping cuts clean and covered until healed o Managing chronic conditions o Recognizing early signs and symptoms of worsening infection and sepsis o Seeking immediate care if signs and symptoms are present
This Sepsis Awareness Month, spread the word about sepsis—you can help save lives.
To learn more about sepsis and how to prevent infections, visit www.cdc.gov/sepsis or call 1-800-CDC-INFO.
From the miscellany department —
Medpage Today offers a special report about a ” New Behavioral Health Database Reveals Gaps in Care — Researchers behind it hope to provide the data needed to remedy the problem.”
STAT News reports “Drug treatment of veterans with opioid use disorder increased during the first year of the pandemic, according to a new study, suggesting that the rapid shift from in-person to telehealth visits at VA medical centers enabled patients to get access to care despite Covid-related disruptions.”
Fierce Healthcare tells us “Cigna’s Evernorth subsidiary is expanding its diabetes care value program to combine traditional pharmaceutical interventions with devices, tools and resources to help patients better understand and manage their diabetes.”
Healthcare Dive informs us that “To staunch the losses of rural hospital closures that endanger access to care for millions, federal regulators are hoping some facilities opt in to a new payment model, but providers say they want more flexibilities and clarity before making the pivot. * * * The new rule ‘maybe gets halfway there,’ Jennifer Findley, vice president of education and special projects at the Kansas Hospital Association, told Healthcare Dive. ‘It’s not as much as we were hoping for but it does give some more flexibility than what you have today.’”
Health Payer Intelligence reports “Chronic diseases are common among emergency department patients, particularly among seniors and those ages 45 to 64, according to a National Health Statistics Report. ‘Monitoring ED visits made by adults at highest risk of severe COVID-19-related illness is important for understanding the health burden of COVID-19 and for planning prevention strategies,’ the researchers explained. ‘Ongoing monitoring of the presence of these underlying chronic conditions at ED visits will continue to inform COVID-19 response efforts.’”
Also Health Payer Intelligence notes that “Three major social determinants of health factors are particularly predominant barriers to care for America’s seniors: economic instability, loneliness, and food insecurity, according to a study sponsored by Alignment Healthcare. Researchers from Toluna conducted an online survey from July 24 to August 13, 2022, which reached 2,600 seniors ages 65 and older. Most respondents identified as white. Half were in Medicare Advantage and this population was divided primarily between preferred provider organizations and health maintenance organizations.”
The Food and Drug Administration on Wednesday [August 31] authorized the first redesign of coronavirus vaccines since they were rolled out in late 2020, setting up millions of Americans to receive new booster doses targeting Omicron subvariants as soon as next week.
The new formulation arrives as roughly 90,000 infections and 475 deaths are still being recorded daily around the United States, more than two years into a pandemic that has killed more than a million Americans and driven a historic drop in life expectancy.
With winter approaching and the BA.5 variant of Omicron still circulating widely, federal officials hope the redesigned shots will help slow the pandemic’s seemingly relentless march. Yet many Americans appear to have become indifferent to the virus and its risks, making the task tougher than ever.
The new boosters are “bivalent,” meaning they contain a combination of the original formulation and one targeting BA.5, now the dominant version of the virus, as well as a sister subvariant of Omicron. One is made by Pfizer and its German partner BioNTech for use in people as young as 12, and the other by Moderna, for those 18 and older.
Here’s a link to the CDC’s 2021 U.S. life expectancy report which was released today.
Advisers to the U.S. Centers for Disease Control and Prevention (CDC) will meet on Thursday [September 1] to vote on whether to recommend the use of two COVID-19 vaccine boosters tailored against the Omicron variant.
A recommendation in favor of the modified vaccines by Pfizer Inc and its German partner BioNTech SE , as well as Moderna Inc is expected to pave the way for a rollout next week.
Medpage Today offers background on tomorrow’s CDC Advisory Committee on Immunization Practices meeting.
ACIP will weigh in on newly authorized fall COVID boosters this week, in a manner unprecedented during the pandemic — without data from human clinical trials.
While most experts agree that there are no safety concerns, and many support the FDA’s attempt to keep up with viral variants, others have pointed out gray areas and open questions when it comes to Omicron-targeting bivalent vaccines.
That includes whether boosters with components targeting Omicron would offer a significant advantage in terms of efficacy — particularly, protection against infection — over boosting against the ancestral strain of the virus alone.
David Leonhardt, writing in his Morning column for the New York Times, provides his latest Covid poll which finds all Americans trending toward placing Covid in the rear view mirror.
A growing number of very liberal Americans have decided that it’s time to treat Covid as an unpleasant but manageable part of life, much as many other Americans — as well as people in other countries — decided months ago.
While the FEHBlog was pleased with the Times poll results, he thinks that Forbes hits the nail on the head with its opinion piece on how America can bring down its Covid death rate which took 383 lives yesterday.
Tragically, the vast majority of Covid-19 deaths are now preventable – if all Americans were up to date with vaccines, and if high-risk individuals got treated promptly after testing positive. If all that were to happen, Covid deaths in the U.S. would be nearly zero, as White House Covid-19 Response Team Coordinator Dr. Ashish Jha told the U.S. Chamber of Commerce Foundation recently.
What can the nation do to make that happen? Put simply, we must embrace the notion that Covid-19 deaths are largely preventable, not inevitable. Instead of trying to put those deaths out of mind, we should focus on what we can do to stop them.
Why are 400 Americans still dying each day? For starters, 15 million seniors have not received their first booster, and only 33% of Americans over 50 and 40% over 65 have received their second booster. In addition, over 20% of adults have not completed their primary vaccination series.
The health impacts of that inaction are sizable. The CDC estimates that among those 50 and older, the unvaccinated had a 29-fold increased risk of dying from Covid-19 and vaccinated people with only one booster had a 4-fold increased risk compared to those with two or more booster doses.
Meanwhile, access to the oral antiviral medication Paxlovid – which reduces the rates at which high-risk people get severe cases of Covid-19 or die from it – is the most limited in zip codes in which people were highly vulnerable to the virus. Moreover, access to and awareness of Evushield – which reduces the risk that immunocompromised people will develop symptomatic Covid-19 for up to six months – remains limited.
To keep Covid-19 and its impact in public consciousness, local health officials should publicly recognize when citizens in their communities lose their lives to the virus. For the same reason, local print and broadcast media should provide coverage of community memorials to those who have died. That should inspire citizens within communities to help each other fully access and use the tools available to all Americans, whether vaccines or treatments.
Local faith organizations, businesses, and other community leaders who have the trust of the population should redouble their efforts reminding individuals that their actions with respect to Covid-19 testing, vaccination, and treatment can make a tangible difference for their community.
Health care professionals should use every office visit, even if unrelated to Covid-19, to remind patients about the need to stay up to date with their vaccinations and have a plan to access treatment if they test positive and are eligible for treatment. The medical community’s attention to preventing and managing chronic conditions such as obesity and diabetes is now even more vital given their detrimental impact on Covid-19 outcomes.
Amen to that. Honestly, while the FEHBlog falls into the senior category, he has been delaying his second booster in order to receive the bivalent vaccine (or the Novovax booster which hasn’t been approved yet). The FEHBlog plans to make an appointment for the bivalent vaccine next week.
Americans may have to pay for their COVID-19 vaccinations as early as January as federal funding for vaccine purchase and distribution runs out and the shots shift to the commercial market, according to Dawn O’Connell, Assistant Secretary for Preparedness and Response at the HHS.
The announcement comes after the HHS hosted over 100 representatives from state and local governments, including various stakeholders, insurers and pharmaceutical companies in a planning meeting on Tuesday.
“While the federal government has been pleased to play this role, we have always known that we would not be in this business forever,” O’Connell said in a post on the ASPR site. “Unfortunately, the timeline to make the transition has accelerated over the past six months without additional funds from Congress to support this work.”
Read that as health plans may have to pay for their members’ Covid vaccinations next year. Conceding that the FEHBlog is not a Hyde amendment expert, he does not understand why the Senate leadership did not ram through more Covid funding in the massive budget reconciliation act.
The Drug Enforcement Administration issued an advisory Tuesday about an “emerging trend” of “brightly-colored” fentanyl pills being used to lure children and young people. What is often called “rainbow fentanyl” has been seized by law enforcement agencies in 18 states just this month, the DEA said.
The drugs, made to look like candy, comes in several forms, including “pills, powder and blocks that resembles sidewalk chalk,” the DEA said.
“Rainbow fentanyl — fentanyl pills and powder that come in a variety of bright colors, shapes, and sizes — is a deliberate effort by drug traffickers to drive addiction amongst kids and young adults,” DEA Administrator Anne Milgram said in a statement.
The US Food and Drug Administration (FDA) said it plans to fight the current opioid crisis by going after online drug retailers and promoting the development of non-opioid alternatives.
On 30 August, the agency published its FDA Overdose Prevention Framework that largely aligns with the Department of Health and Human Service’s (HHS) 2021 Overdose Prevention Strategy. The framework echoes concepts in the HHS strategy, such as supporting primary prevention, encouraging harm reduction and advancing evidence-based treatments. FDA’s framework also includes the actions to protect the public from unapproved, diverted and counterfeit drugs with overdose risk.
In a blog post, FDA Commissioner Robert Califf said the agency needs new approaches to counter the rapid growth of illicit, chemically synthesized fentanyl, fentanyl analogs and methamphetamines on the market. Cracking down on such activities while securing the supply chain for approved opioids and other controlled substances is a top priority, he said.
In U.S. healthcare business news, Healthcare Dive reports
Walgreens Boots Alliance has completed its majority stake acquisition in at-home care technology platform CareCentrix, the retail pharmacy giant announced Wednesday.
The $330 million investment gives Walgreens a 55% ownership of CareCentrix. Walgreens has the option to acquire the remaining equity in the future.
The investment, first announced in October, expands Walgreen’s reach in the health sector, especially in the areas of primary care, specialty pharmacy, post-acute and home care, the company said in a Wednesday release.
Employers, who provide health coverage to roughly half the U.S. population, are acutely aware of where health care’s current cost trajectory is headed. In a recent survey of executives at 300 of the country’s largest employers, nearly 90% said they believe the cost of providing health benefits will become unsustainable within five to 10 years.
Yet instead of finding new ways to manage costs and help sustain this critical lifeline for America’s workers, many health systems continue to increase the prices they charge commercial insurers. And they can because, in many cases, newly consolidated health systems are the only game in town.
Employers and private insurers pay, on average, 224% of what Medicare would have paid for the same service at the same facility, despite new data showing that hospitals require payments that represent just 127% of Medicare to cover their expenses.
In federal employee compensation news, Federal News Network reports
President Joe Biden has formally announced his plans to give civilian federal employees a pay raise next year, starting on Jan. 1, 2023.
The president is specifically recommending a 4.1% across-the-board pay raise for federal employees in 2023, with an additional 0.5% average locality pay adjustment — resulting in a 4.6% average pay increase.
Biden said his alternative pay plan would help federal pay stay competitive with what workers with critical skills could earn in the private sector.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.