The FEHBlog wishes all of his readers a Happy New Year.
The Wall Street Journal reports that in the wake of the December 29 D.C. Circuit opinion upholding the Trump Administration’s hospital price transparency rule,
The nation’s largest hospital chains, including publicly traded giants HCA Healthcare Inc., Universal Health Services Inc. and Community Health Systems Inc., and national nonprofit chains CommonSpirit Health and Ascension, said they planned to comply with new requirements to post pricing. Tenet Healthcare Corp. declined to comment.
“Ascension supports price transparency of our hospital services for the benefit of consumer choice and access to care for those we serve,” said Nick Ragone, a spokesman for the St. Louis-based chain.
As of Jan. 1, hospitals will be required to publish the prices negotiated privately with each payer for 300 common services for easy use by consumers, and make public the same information for all their procedures in a format that can be read and analyzed by computers.
The FEHBlog will be back on January 2 for Saturday Stats and More. Enjoy.
Per the Office of Personnel Management, “The effective date of the Open Season change is the first day of the first full pay period in January. For annuitants this date will always be January 1.” It turns out that Sunday January 3, 2021, is the first day of the first full pay period in January 2021. How convenient.
The Consolidated Appropriations Act, 2021, does include the three standard FEHBP appropriations provisions — a prohibition on applying full Cost Accounting Standards coverage to FEHB contracts (Sec. 611), an abortion coverage restriction (Secs. 613, 614), and a limited contraceptive coverage mandate (Sec. 726) which the Affordable Care Act has overridden. What’s more this new law extends the option of FEHBP and FEGLI coverage to 120 tribal grant schools thereby filling a coverage gap erroneously created by the Affordable Care Act. This option is exercised by the tribal employers who must make the minimum federal civil servant government contribution toward the benefit coverage.
For the past 20 years or so, the FEHBP has offered plan members transitional care protection pursuant to President Clinton’s Bill of Consumer Rights which states in pertinent part as follows:
Consumers who are undergoing a course of treatment for a chronic or disabling condition (or who are in the second or third trimester of a pregnancy) at the time they involuntarily change health plans or at a time when a provider is terminated by a plan for other than cause should be able to continue seeing their current specialty providers for up to 90 days (or through completion of postpartum care) to allow for transition of care.
FEHB plan carriers intending to terminate a network provider for cause generally could comply with this requirement by giving affected members 90 days advance notice of the change.
It turns out that Section 113 Division BB of the Consolidated Appropriations Act, 2021, includes an Affordable Care Act amendment ensuring continuity of care. The requirements of this new law bear similarities to the FEHBP’s transitional care protections. However, as always, the devil is in the details. For example, the new law’s transitional care provisions apply to any provider contract termination, including passive non-renewals, whether triggered by the provider or the payer, with the limited exception of payer termination for fraud or failure to meet applicable quality standards. FEHB plans and OPM have a year to sort out the details before the new requirements take effect on January 1, 2022.
In other news —
The Senate moved forward today on overriding President’s veto of the FY 2021 National Defense Authorization Act but not on the $2000 COVID-19 relief direct stipend per the Wall Street Journal:
Moving through the procedural steps for overriding Mr. Trump’s veto of the National Defense Authorization Act could take up much of the Senate’s time before Sunday. Sen. Bernie Sanders (I., Vt.), in a push for a stand-alone vote on increasing the size of the direct checks, has stopped Mr. McConnell from fast-tracking votes on the NDAA override. As a result, the final vote on the NDAA may not take place until Saturday due to a series of procedural steps.
The Senate took one of those steps late Wednesday, voting 80-12 to move forward with the bill, in another show of broad, bipartisan support for the legislation Mr. Trump vetoed.
Bleeping Computer updated us on how the federal government is addressing the SolarWinds backdoor hack.
The Cybersecurity and Infrastructure Security Agency (CISA) has ordered all US federal agencies to update the SolarWinds Orion platform to the latest version by the end of business hours on December 31, 2020. CISA’s Supplemental Guidance to Emergency Directive 21-01 demands this from all agencies using Orion versions unaffected in the SolarWinds supply chain attack.
The U.S. Court of Appeals for the District of Columbia Circuit issued an opinion today affirming a district court holding that the Trump Administration’s hospital price transparency rule is lawful. The rule takes effect on Friday January 1. Needless to say the Court also denied the appellant American Hospital Association’s motion for an emergency stay of the rule.
On a similar note, one of the transparency provisions included in the Consolidated Appropriations Act, 2021, amendments to the Affordable Care Act (Section 114 of Division BB) states:
‘‘A group health plan or a health insurance issuer offering group or individual health insurance coverage shall offer price comparison guidance by telephone and make available on the Internet website of the plan or issuer a price comparison tool that (to the extent practicable) allows an individual enrolled under such plan or coverage, with respect to such plan year, such geographic region, and participating providers with respect to such plan or coverage, to compare the amount of cost-sharing that the individual would be responsible for paying under such plan or coverage with respect to the furnishing of a specific item or service by any such provider.’’’
This new requirement, which applies to FEHB plans, takes effect with the first plan year beginning on or after January 1, 2022. The recently finalized Trump Administration’s payer transparency rule kicks in a year later. We will have to see how the Biden Administration handle this.
As the FEHBlog just picked up a couple of delicious Christmas cookies, it is time to consider the joint HHS and Department of Agriculture Dietary Guidelines for Americans 2020-2025 released today. The announcement described the publication as “the nation’s trusted resource for evidence-based nutrition guidance. The guidelines are designed for use by healthcare professionals and policy makers for outreach to the general public and provide the nutritional foundation for federal nutrition programs. The dietary guidelines should not be considered clinical guidelines for the treatment of disease.” The announcement notes that
Steeped in scientific evidence, the key recommendations look similar to those of the past and address two topics that garnered much attention throughout the development of the guidelines – added sugars and alcoholic beverages. Dietary Guidelines for Americans, 2020-2025 carried forward the committee’s emphasis on limiting these dietary components, but did not include changes to quantitative recommendations, as there was not a preponderance of evidence in the material the committee reviewed to support specific changes, as required by law. As in previous editions, limited intake of these two food components is encouraged. In fact, this sentiment remains prominent throughout the policy document and complements
For consumers, USDA’s MyPlate translates and packages these principles of dietary guidance for Americans in a way that is handy and accessible. To share these messages broadly, USDA offers the Start Simple with MyPlate campaign and a new MyPlate websiteto help individuals, families, and communities make healthy food choices that are easy, accessible, and affordable, in addition to helping prevent chronic disease. For more information, please visit www.myplate.gov.
Funny, the FEHBlog no longer sees Christmas cookies on his plate.
P.S. The Senate did not vote on the stipend increase or the NDAA veto today per the Wall Street Journal. This session of Congress ends on Saturday.
Today, the House of Representatives voted 322-87 to override the President’s veto of the Fiscal Year 2021 National Defense Authorization Act. Govexec notes that “The NDAA contains several provisions for federal employees, such as making technical corrections to the paid parental leave policy from last year’s bill and waiving the normal annual cap for unused leave from year to year.” The Senate is expected to complete the veto action in a vote tomorrow. This would be the first time that Congress has overridden one of President Trump’s vetoes.
The House of Representatives also voted in favor of a “clean bill” to amend the latest COVID-19 relief law (H.R. 133) by increasing the direct stipend from $600 to $2000 per person. That bill now goes to the Senate.
The FEHBlog noted earlier this month that the American Hospital Association had asked Congress not to disrupt payer / provider network contracting in the COVID-19 relief bill. Of course, the surprise billing restrictions may encourage in-network providers to make the jump to out-of-network status particularly if the surprise billing arbitration decisions favor the providers. Time will tell on that one, but the following ACA amendment in H.R. 133 reminded the FEHBlog of the AHA’s warning.
Division BB, SEC. 108. IMPLEMENTING PROTECTIONS AGAINST PROVIDER DISCRIMINATION.
Not later than January 1, 2022, the Secretary of Health and Human Services, the Secretary of Labor, and the Secretary of the Treasury shall issue a proposed rule implementing the protections of section 2706(a) of the Public Health Service Act (42 U.S.C. 300gg-5(a)). The Secretaries shall accept and consider public comments on any proposed rule issued pursuant to this subsection for a period of 60 days after the date of such issuance. Not later than 6 months after the date of the conclusion of the comment period, the Secretaries shall issue a final rule implementing the protections of section 2706(a) of the Public Health Service Act
Congress has set the fuse on another one of the Affordable Care Act’s time bombs directed at provider networks. Section 2706(a) reads as follows:
A group health plan and a health insurance issuer offering group or individual health insurance coverage shall not discriminate with respect to participation under the plan or coverage against any health care provider who is acting within the scope of that provider’s license or certification under applicable State law. This section shall not require that a group health plan or health insurance issuer contract with any health care provider willing to abide by the terms and conditions for participation established by the plan or issuer. Nothing in this section shall be construed as preventing a group health plan, a health insurance issuer, or the Secretary from establishing varying reimbursement rates based on quality or performance measures.
The Obama Administration on April 29, 2013, issued the following ACA FAQ on this law:
Q2: Will the Departments be issuing regulations addressing PHS Act section 2706(a) prior to its effective date?
No. The statutory language of PHS Act section 2706(a) is self-implementing and the Departments do not expect to issue regulations in the near future. PHS Act section 2706(a) is applicable to non-grandfathered group health plans and health insurance issuers offering group or individual health insurance coverage for plan years (in the individual market, policy years) beginning on or after January 1, 2014.
Until any further guidance is issued, group health plans and health insurance issuers offering group or individual coverage are expected to implement the requirements of PHS Act section 2706(a) using a good faith, reasonable interpretation of the law. For this purpose, to the extent an item or service is a covered benefit under the plan or coverage, and consistent with reasonable medical management techniques specified under the plan with respect to the frequency, method, treatment or setting for an item or service, a plan or issuer shall not discriminate based on a provider’s license or certification, to the extent the provider is acting within the scope of the provider’s license or certification under applicable state law. This provision does not require plans or issuers to accept all types of providers into a network. This provision also does not govern provider reimbursement rates, which may be subject to quality, performance, or market standards and considerations.
The Departments will work together with employers, plans, issuers, states, providers, and other stakeholders to help them come into compliance with the provider nondiscrimination provision and will work with families and individuals to help them understand the law and benefit from it as intended.
The FEHBlog recalls that ancillary providers such as chiropractors were particularly exercised by, and insurers were relieved by, the Administration’s statement that “This provision does not govern provider reimbursement rates, which may be subject to quality, performance, or market standards and considerations.” While the statute does not expressly mention consideration of “market standards and considerations,” such a fine point has not stopped federal agencies from elaborating on statutory standards in the past. The FEHBlog expects that this mandated rule making will be a tug of war over statutory interpretation that will wind up in the courts If the providers win this tug of war and the surprise billing arbitrations, then healthcare spending will resume its upward curve.
And there’s more to follow tomorrow. If you want to find the text of H.R. 133 visit this Congress.gov website and download the PDF of the enrolled bill. The ACA amendments may be found in Division BB. You can search for Division BB using the Adobe Acrobat find tool.
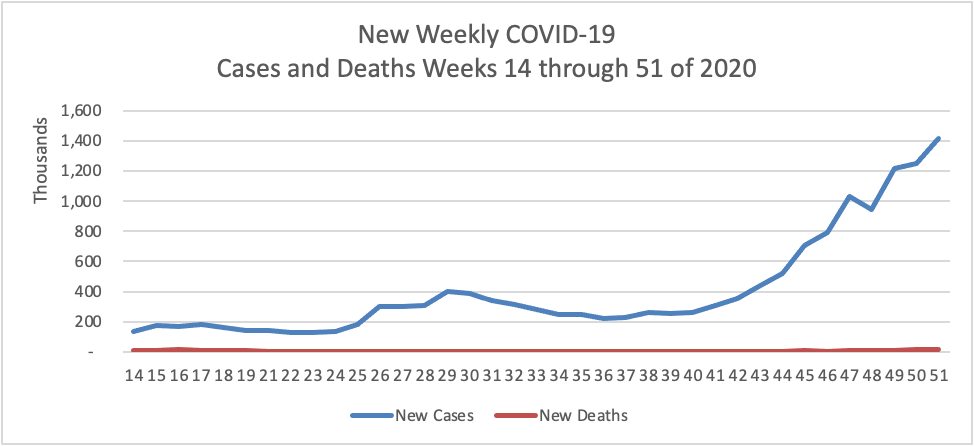
Based on the CDC’s Cases in the U.S. website, here is the FEHBlog’s chart of new weekly COVID-19 cases and deaths over the 14th through 51st weeks of this year (beginning April 2 and ending December 23; using Thursday as the first day of the week in order to facilitate this weekly update):
and here is the CDC’s latest overall weekly hospitalization rate chart for COVID-19:
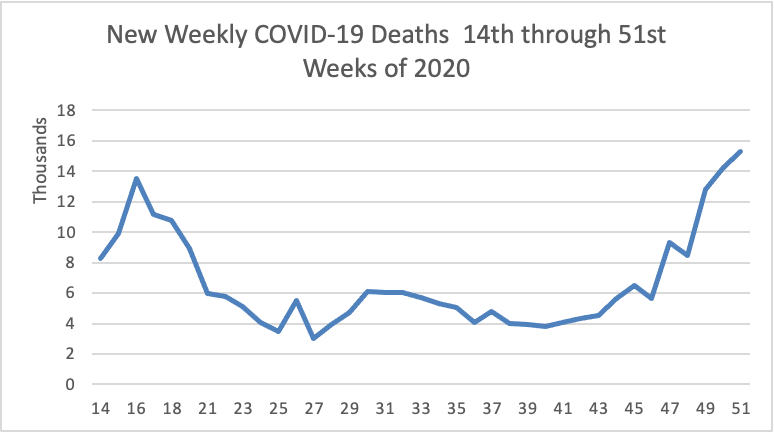
The FEHBlog has noted that the new cases and deaths chart shows a flat line for new weekly deaths because new cases greatly exceed new deaths. Accordingly here is a chart of new COVID-19 deaths over the period (April 2 through December 23):
The latest CDC FluView will be available on Monday December 28. Next week the FEHBlog will begin to include COVID vaccines in these charts.
The FEHBlog had planned to start reviewing the Affordable Care Act changes in the Consolidated Appropriations Act, 2021, but because the status of that bill unfortunately is in limbo, he instead will note two other Congressionally passed bills that are expected to receive the President’s signature:
The McCarran-Ferguson Act of 1945 “limited the application of [federal] antitrust laws to the business of insurance as long as and to the extent state law regulated the business of insurance. However, if states would not regulate insurance, the Sherman and Clayton Acts, as well the Federal Trade Commission Act still applied.” Needless to say the States with the assistance of the National Association of Insurance Commissioners made sure that the States did not unwittingly create such a regulatory gap. In any event. the McCarran- Ferguson Act continued to apply federal anti-trust law, specifically the Sherman Act of 1896, to prohibit “any agreement to boycott, coerce, or intimidate, or act of boycott, coercion, or intimidation” (15 U.S.C. Sec. 1013).
H.R. 1418 adds to the McCarran- Ferguson Act a further exception for health insurance, dental insurance and limited scope dental benefits. In other words health insurers and dental insurers will be subject to both federal and state laws against restraint of trade. The garden variety exceptions to extension of federal anti-trust law appear quite narrow to the FEHBlog.
“(A) to collect, compile, or disseminate historical loss data; (B) to determine a loss development factor applicable to historical loss data; (C) to perform actuarial services if such contract, combination, or conspiracy does not involve a restraint of trade; or (D) to develop or disseminate a standard insurance policy form.”
Matt Eyles, president of America’s Health Insurance Plans (AHIP), said in a statement about passage of H.R. 1418 that implementation of the bill would add layers of bureaucracy to health insurers and destabilize markets.
“Removal of this exemption adds tremendous administrative costs while delivering absolutely no value for patients and consumers,” Eyles said.
Consumer Reports put out a commentary welcoming passage of H.R. 1418.
“The antitrust exemption has essentially allowed health insurers to act as a monopoly, making demands in lockstep on the terms they will offer consumers and health care providers,” the advocacy organization said in a comment on bill passage. “The resulting squeeze puts pressure on providers to cut corners on service in order to increase the profits the health insurers can extract.”
How much can insurers extract when those profits are strictly regulated by the Affordable Care Act?
This bill, which the FEHBlog previously has mentioned, requires HHS’s Office for Civil Rights to consider whether the covered entity or business associate has adequately demonstrated that it had, for not less than the previous 12 months, recognized security practices in place, when imposing penalties or other remedies for HIPAA Security Rule violations.
The bill defines “Recognized security practices” to mean
the standards, guidelines, best practices, methodologies, procedures, and processes developed under section 2(c)(15) of the National Institute of Standards and Technology Act, the approaches promulgated under section 405(d) of the Cybersecurity Act of 2015, and other programs and processes that address cybersecurity and that are developed, recognized, or promulgated through regulations under other statutory authorities. Such practices shall be determined by the covered entity or business associate, consistent with the HIPAA Security rule (part 160 of title 45 Code of Federal Regulations and subparts A and C of part 164 of such title).
The bill expressly does not create liability for HIPAA covered entities and business associates which decide not to adopt such practices. The bill is retroactive to the effective date of the 21st Century Cures Act of 2016.
In other healthcare legal news:
Reuters reports that on December 23, 2020, a federal district judge in Maryland “blocked a last-minute Trump administration rule aimed at lowering drug prices as of next week. The rule, scheduled to take effect on Jan. 1, would have tied reimbursements for 50 drugs by Medicare, a U.S. government insurance program, to the lowest prices paid by certain other countries. U.S. District Judge Catherine Blake in Maryland ruled that the administration had rushed the rule without giving the public a chance to comment, in violation of federal law.” Case No. 1:20-cv-03531 (D. Md). The temporary restraining order is effective for 14 days.
The American Hospital Association, along with several other organizations, filed an emergency stay of enforcement motion to prevent the Department of Health and Human Services’ hospital price transparency rule from going into effect Jan. 1. The rule requires each hospital operating in the U.S. to make public pricing information, including the prices they negotiate with commercial health insurers. Last week, the Centers for Medicare and Medicaid issued a bulletin announcingits plans to audit a sample of hospitals for compliance with the rule starting in January.
The motion was filed with the U.S. Court of Appeals for the D.C. Circuit in its appeal of a lower court order affirming the legality of this rulemaking (Case No. 20-5193). In its opposition to this motion, the Justice Department observed that
This Court granted plaintiffs’ request for an expedited briefing and argument schedule to “allow the Court to hear and decide this case before” January 1, 2021. Pls. Mot. to Expedite, at 5 (July 3, 2020). The Court is likely to rule on the merits of this appeal imminently, thereby resolving plaintiffs’ legal challenge. Should the Court affirm the district court’s rejection of plaintiffs’ claims, plaintiffs would not be entitled to any relief, including a stay of the agency’s rule. Should the Court agree with plaintiffs’ legal challenge, by contrast, plaintiffs would be entitled to appropriate relief.
The FEHBlog will keep an eye out for this opinion next week.
The Continuing Appropriations Act, 2021, includes hundreds of pages of amendments to the Affordable Care Act. The premier change is the No Surprises Act which is principally a patient protection measure. NPR lays out this new law’s requirements which take effect for plan years beginning on or after January 1, 2022.
Over the remaining posts of 2020, the FEHBlog will point out other new health plan obligations for 2022 created by this bill, which the President will sign into law within the week. Many of those provisions were drawn from the Senate Health Education and Labor Committee’s S. 1785 from the last Congress. Suffice it to say that 2021 will be very busy year for health plans and their vendors.
Federal News Network discusses how the Continuing Appropriations Act, 2021, impacts federal government agencies and their employees. Of note, the bill
“silent[ly] endorse[s] the president’s 1% across-the-board federal pay raise for civilian employees in 2021;”
“allow[s} those subject to the president’s payroll tax deferral to pay back the deferred taxes — worth 6.2% of their income — throughout the entire year of 2021;”
“appropriates to the Office of Personnel Management $36 million more [in the current federal fiscal year] to make up for the revenue it lost when it transferred the governmentwide security clearance business to the Defense Department,” and
“contains a provision requiring OPM to establish a new occupational series for artificial intelligence positions, or update an existing series to more accurately account for those kinds of skills needed in the federal government.”
On the COVID-19 front, Kaiser Health News helpfully gathers stories about the variant of the COVID-19 virus that recently cropped up in Britain. Fierce Healthcare adds
Moderna * * * said in a statement provided to other media outlets that it expects “that the Moderna vaccine-induced immunity would be protective against the variants recently described in the U.K.,” and that it “will be performing additional tests in the coming weeks to confirm this expectation.”
Pfizer pointed out that when SARS-CoV-2, the virus that causes COVID-19, first emerged a year ago, it was clear there was more than one strain of it, and that it was mutating as it spread. SARS-CoV-2 is an RNA virus, and as such, it has “exceptionally high [mutation] rates” because the enzymes it uses for replication are “prone to errors when making new virus copies,” the company said.
“One of the reasons Pfizer and BioNTech chose to utilize a mRNA platform is because of the potential for the flexibility of the technology in comparison to traditional vaccine technologies,” including the ability to change the RNA sequence in the vaccine, should a strain emerge that’s not covered by the current shot,” Pfizer added.
Both COVID-19 vaccine manufacturers urged public calm.
In October 2020, the FEHBlog noted that Walmart preemptively had sued the federal government over its opioid crisis policy shortcomings. Nevertheless the other shoe dropped today when the federal government sued Walmart in Delaware’s federal court.. According to Justice Department’s press release.
In a civil complaint filed today, the Department of Justice has alleged that Walmart Inc. unlawfully dispensed controlled substances from pharmacies it operated across the country and unlawfully distributed controlled substances to those pharmacies throughout the height of the prescription opioid crisis.
The complaint alleges that this unlawful conduct resulted in hundreds of thousands of violations of the Controlled Substances Act (CSA). The Justice Department seeks civil penalties, which could total in the billions of dollars, and injunctive relief.
Lawmakers raced to put finishing touches on a roughly $900 billion coronavirus aid package, pushing up against a midnight deadline to complete the agreement and pass it through Congress.
With a disagreement on the Federal Reserve’s emergency lending powers settled earlier in the weekend, negotiators on Sunday were finalizing details for the rest of the bill. Senate Majority Leader Mitch McConnell (R., Ky.) said Sunday afternoon that negotiators were hours away from completing the deal. * * *
The emerging agreement is expected to provide $300 a week in enhanced federal unemployment benefits, a $600 direct check to many Americans, as well as aid for schools, vaccine distribution and small businesses. Final votes in the House and Senate could occur as early as Sunday.
Lawmakers raced to put finishing touches on a roughly $900 billion coronavirus aid package, pushing up against a midnight deadline to complete the agreement and pass it through Congress.
With a disagreement on the Federal Reserve’s emergency lending powers settled earlier in the weekend, negotiators on Sunday were finalizing details for the rest of the bill. Senate Majority Leader Mitch McConnell (R., Ky.) said Sunday afternoon that negotiators were hours away from completing the deal. * * *
The emerging agreement is expected to provide $300 a week in enhanced federal unemployment benefits, a $600 direct check to many Americans, as well as aid for schools, vaccine distribution and small businesses. Final votes in the House and Senate could occur as early as Sunday.
The House is expected to vote on a 24-hour extension of government funding Sunday evening, setting up votes on the relief agreement and broader spending bill for Monday. The aid package is tied to a roughly $1.4 trillion annual spending package and Congress has passed a series of temporary spending bills in recent days to keep the government funded while it finished the negotiations.
Significantly, Politico reports that “Congress is set to include a long-elusive ban on “surprise” medical bills as part of a major spending deal lawmakers were working to finalize Sunday evening.”
(P.S. Govexec.com confirms that Congress passed a one day extension of the continuing resolution Sunday night.)
On the COVID-19 front —
The Centers for Disease Control now has a COVID-19 vaccines website which indicates that as of 1 pm today 2,838,225 doses of vaccine have been distributed and 556,208 doses have been administered in the first week.
In accordance with CDC Advisory Committee on Immunization Practices recommendations, the current phase 1A of distribution is directed at healthcare personal and nursing home residents, The Wall Street Journal reports that ACIP today approved phases 1B and 1C as follows:
The next group would include people ages 75 and older, whose hospitalization and death rates are the highest of all age groups. It would also include teachers, factory workers, police and firefighters, grocery store workers and others who are considered essential to the functioning of the economy and at high risk of exposure to Covid-19.
Another group would follow them, comprised of people between the ages of 65 and 74, anyone age 16 or over with a medical condition that puts them at high risk of complications from Covid-19, and other essential workers. They include people who work in transportation and logistics, food service, water and wastewater, and energy sectors.
The ACIP vote was 13-1. State governors are the ultimate decision makers in their states but the FEHBlog understands the governors generally defer to ACIP. As the FEHBlog has noted the vaccines are being directly distributed to federal agencies too.
On the COVID-19 treatment front, the Wall Street Journal reports that
Doctors are treating a new flood of critically ill coronavirus patients with treatments from before the pandemic, to keep more patients alive and send them home sooner.
Last spring, with less known about the disease, doctors often pre-emptively put patients on ventilators or gave powerful sedatives largely abandoned in recent years. The aim was to save the seriously ill and protect hospital staff from Covid-19.
Now hospital treatment for the most critically looks more like it did before the pandemic. Doctors hold off longer before placing patients on ventilators. Patients get less powerful sedatives, with doctors checking more frequently to see if they can halt the drugs entirely and dialing back how much air ventilators push into patients’ lungs with each breath.
“Let us go back to basics,” said Dr. Eduardo Oliveira, executive medical director for critical-care services for AdventHealth Central Florida, which recommends its doctors stick with pre-pandemic guidelines for ventilator use. “The less you deviate from it, the better.”
Advances also include new drugs, most notably steroids, for severely ill patients.
In other healthcare news, Health Payer Intelligence informs us that
Payers may consider promoting ambulatory surgery centers as the ideal site of care for joint replacement surgeries, UnitedHealth Group’s recent research findings suggested.
“Findings from new UnitedHealth Group research underscore the importance of optimizing sites of care to improve patient safety and reduce costs,” the report summarized.
The study analyzed data 2018 and 2019 procedures conducted at Optum’s ambulatory surgery centers. The researchers used low- and medium-severity surgeries to from the baseline and gauge shifts in costs and savings. They used the Ambulatory Surgery Centers Quality Collaboration’s recommended outcome measures to assess quality of care.
On the SolarWinds backdoor hack front, check out this ArsTechnica article:
Of the 18,000 organizations that downloaded a backdoored version of software from SolarWinds, the tiniest of slivers—possibly as small as 0.2 percent—received a follow-on hack that used the backdoor to install a second-stage payload. The largest populations receiving stage two were, in order, tech companies, government agencies, and think tanks/NGOs. The vast majority—80 percent—of these 40 chosen ones were located in the US.
These figures were provided in an update from Microsoft President Brad Smith. Smith also shared some insightful and sobering commentary on the significance of this almost unprecedented attack. His numbers are incomplete, since Microsoft sees only what its Windows Defender app detects. Still, Microsoft sees a lot, so any difference with actual numbers is likely a rounding error.
The FEHBlog had been wondering why not all of the victims of the backdoor hack were breached. It was a conscious decision by the hackers.
Based on the CDC’s Cases in the U.S. website, here is the FEHBlog’s chart of new weekly COVID-19 cases and deaths over the 20th through 50th weeks of this year (beginning May 14 and ending December 16; using Thursday as the first day of the week in order to facilitate this weekly update):
and here is the CDC’s latest overall weekly hospitalization rate chart for COVID-19:
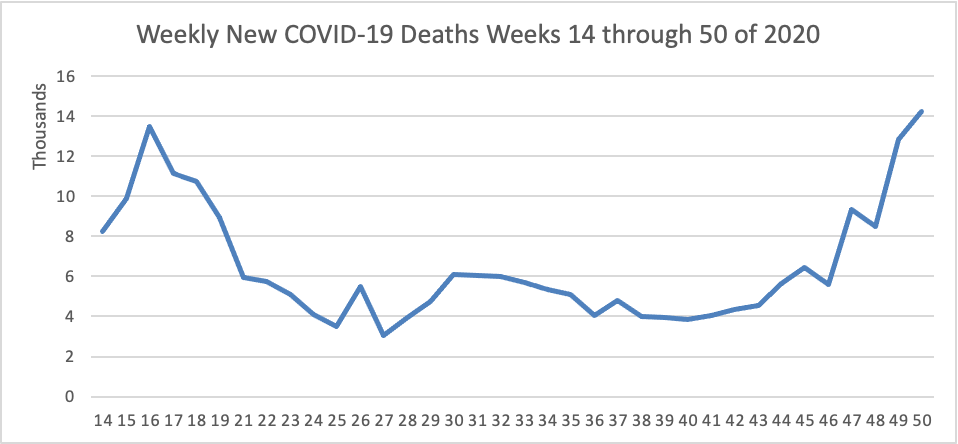
The FEHBlog has noted that the new cases and deaths chart shows a flat line for new weekly deaths because new cases greatly exceed new deaths. Accordingly here is a chart of new COVID-19 deaths over the period (April 2 through December 9). The FEHBlog extended this chart from April 2 to May 14 in order to display the previous high for this sad metric.
The CDC’s current Fluview report continues to state “Seasonal influenza activity in the United States remains lower than usual for this time of year.” So Americans must be doing something right.
1) substantial increases in drug overdose deaths across the United States, primarily driven by rapid increases in overdose deaths involving synthetic opioids excluding methadone (hereafter referred to as synthetic opioids), likely illicitly manufactured fentanyl; (2) a concerning acceleration of the increase in drug overdose deaths, with the largest increase recorded from March 2020 to May 2020,coinciding with the implementation of widespread mitigation measures for the COVID-19 pandemic; (3) the changing geographic distribution of overdose deaths involving synthetic opioids, with the largest percentage increases occurring in states in the western United States; (4) significant increases in overdose deaths involving psychostimulants with abuse potential (hereafter referred to as psychostimulants) such as methamphetamine; and
The House [of Representatives] passed a two-day spending bill Friday evening, sending it over to the Senate in a bid to prevent a partial government shutdown after midnight, as congressional leaders struggled to wrap up negotiations on a coronavirus relief package.
In the Covid-19 talks, negotiators were still wrestling Friday to close differences on the Federal Reserve’s emergency lending powers among other final snags. Leaders have aimed to pair the passage of the Covid-19 aid bill with a broader spending bill.
The FEHBlog expected a little bit longer extension but a two day extension suggests that the compromise on the COVID-19 relief bill is near. The FEHBlog cannot believe that with the Georgia Senate primary approaching on January 5 that either party would risk a government shutdown or not COVID-19 relief. But we shall see.
In that regard, the FEHBlog read on the American Hospital Association’s daily report about this health system letter to Congress, delivered today, suggesting that there is some crazy language in that bipartisan surprise billing proposal. Again, we shall see.
HHS’s Office for Civil Rights issued “guidance on how the Health Insurance Portability and Accountability Act of 1996 (HIPAA) permits covered entities and their business associates to use health information exchanges to disclose protected health information (PHI) for the public health activities of a public health authority. The guidance provides examples relevant to the COVID-19 public health emergency on how HIPAA permits covered entities and their business associates to disclose PHI to an HIE for reporting to a PHA that is engaged in public health activities.”
It’s the 250th anniversary of the birth of that great composer Ludwig van Beethoven. Speaking of birthdays, the FEHBlog heard today that Dr. Anthony Fauci turns 80 on December 24. According to the Washington Post, he is urging Americans to have a merry little Christmas. Touche.
On the omnibus/COVID-19 relief bill front, Bloomberg reports that
Congressional leaders are still haggling over the final details of nearly $900 billion in coronavirus aid as staff members try to write the legislative language needed for House and Senate votes this week.
If the aid deal, combined with a spending bill needed to fund the government, isn’t ready to get a vote in both chambers by Friday, another stopgap measure will be needed to avert a partial government shutdown after midnight Friday.
People briefed on the negotiations say the draft of the plan includes $600 in payments for individuals, $300-per-week in supplemental unemployment insurance payments and aid for small businesses, but it omits aid to state and local governments and lawsuit liability protection. It also includes roughly $17 billion for airlines.
Senate Majority Leader Mitch McConnell, House Speaker Nancy Pelosi, Senate Democratic leader Chuck Schumer and House Republican leader Kevin McCarthy continued negotiations on Wednesday, although the deal is more likely to come together by Thursday, according to a lawmaker briefed on the talks.
The FEHBlog expected the legislative language today but good things come to those who wait, right?
The CMS actuary released his annual report on the previous year’s healthcare spending. “Total national healthcare spending in 2019 grew 4.6%, which was similar to the 4.7% growth in 2018 and the average annual growth since 2016 of 4.5%.” 2020 may be the outlier.
HHS began distributing the third phase of COVID-19 relief funding for providers Wednesday, with $24.5 billion to go to more than 70,000 providers through the end of January. The amount exceeds the original $20 billion planned for this tranche as officials realized more would be needed to get providers close to whole from coronavirus-related losses. HHS said up to 88% of applicants’ reported losses are being reimbursed.
In that regard, Fierce Healthcare reports that major healthcare systems which own a health insurer are weathering the COVID-19 storm better than most health systems according to a PwC report. “PwC pointed to major health systems such as Intermountain, Kaiser Permanente and Presbyterian Healthcare Services that used health plans to help bolster their finances.” It’s not surprising to the FEHBlog that hedges like this work. Large health insurers similarly are acquiring healthcare providers.
In other news —
The EEOC offers guidance for employers who want to make sure that their employee are vaccinated again COVID-19 and also want to comply with federal anti-discrimination law. This new guidance is Q&A K.
EHR Intelligence discusses the Gravity Project’s efforts to introduce social determinants of health data into electronic health records.
Health Payer Intelligence informs us about a PwC Health Research Institute report concluding that “Payers and stakeholder collaborators have the opportunity to rebuild the healthcare system into a more effective and consumer-centric system in 2021 by honing virtual care and other strategies.”
Krebs on Security details the malicious hack on the SolarWinds/Orion platform used by federal agencies and Fortune 500 companies “to monitor the health of their IT networks.”
Becker’s Health IT reports that “Healthcare workers in Indiana who tried signing up for the first round of COVID-19 vaccinations Dec. 14 overwhelmed the state’s enrollment website, resulting in down time, according to Indianapolis NBC affiliate WTHR.” Why is this good news? Because now that the COVID-19 vaccine is a reality, people will want the jab as the call it in Britain. That’s human nature.
The Wall Street Journal reports that “The Food and Drug Administration [“FDA’] said Tuesday that the Covid-19 vaccine developed by Moderna Inc. was “highly effective,” setting the stage for an emergency authorization later this week that would add a second vaccine to the arsenal against the pandemic.” Here’s a link to the Moderna briefing document for Thursday’s meeting with the FDA’s Vaccines and Related Biological Products Advisory Committee.
A friend of the FEHBlog pointed out the following encouraging FDA announcement
Today, the U.S. Food and Drug Administration issued an emergency use authorization (EUA) for the first over-the-counter (OTC) fully at-home diagnostic test for COVID-19. The Ellume COVID-19 Home Test is a rapid, lateral flow antigen test, a type of test that runs a liquid sample along a surface with reactive molecules. The test detects fragments of proteins of the SARS-CoV-2 virus from a nasal swab sample from any individual 2 years of age or older.
“Today’s authorization is a major milestone in diagnostic testing for COVID-19. By authorizing a test for over- the-counter use, the FDA allows it to be sold in places like drug stores, where a patient can buy it, swab their nose, run the test and find out their results in as little as 20 minutes,” said FDA Commissioner Stephen M. Hahn, M.D. “As we continue to authorize additional tests for home use, we are helping expand Americans’ access to testing, reducing the burden on laboratories and test supplies, and giving Americans more testing options from the comfort and safety of their own homes.”
The announcement today of the first fully at-home OTC COVID-19 diagnostic test follows last month’s authorization of the first prescription COVID-19 test for home use and last week’s announcement of the first non-prescription test system, in which a lab processes the self-collected sample. The FDA has authorized more than 225 diagnostic tests for COVID-19 since the start of the pandemic, including more than 25 tests that allow for home collection of samples, which are then sent to a lab for testing. The Ellume COVID-19 Home Test is the first COVID-19 test that can be used completely at home without a prescription.
On the omnibus / COVID-19 relief bill front, the Wall Street Journal reports
The top four congressional leaders discussed a coronavirus relief package and sweeping spending bill on Tuesday and planned to return for another meeting in the evening, as lawmakers raced to reach an agreement before critical support programs expire at year’s end.
House Speaker Nancy Pelosi (D., Calif.), Senate Majority Leader Mitch McConnell (R., Ky.), Senate Minority Leader Chuck Schumer (D., N.Y.) and House Minority Leader Kevin McCarthy (R., Calif.) first conferred in the afternoon, with the meeting of both parties’ leaders a signal that they could be ready to make the difficult decisions needed to cut a deal.
The group will meet again late Tuesday.
“We’re continuing to work. I think there’s progress. We’ll get back together,” Mr. McCarthy said following the afternoon meeting.
Treasury Secretary Steven Mnuchin, who spoke to Mrs. Pelosi earlier Tuesday for more than an hour, also joined the first meeting by phone.
The legislative text must be released tomorrow if Congress want to stick with the current December 18 deadline for action.
A friend of the FEHBlog pointed out the Office of Management and Budget’s Office of Information and Regulatory Affairs has issued its Fall 2020 Unified Agenda of “Regulatory and Deregulatory Actions. Here’s a link to the OPM agenda. The FEHBlog noticed a FEHBP centralized enrollment proposed rule and a final FEHBAR rule involving the Truth in Negotiations Act threshold change which the FEHBlog called to OPM’s attention.
In other healthcare news
Health Payer Intelligence offers “Five Pivotal Payer Industry Trends To Watch in 2021.”
Healthcare Finance News reports that various healthcare trade associations have asked a federal district court in Maryland to preliminarily enjoin implementation of the Trump Administration’s Medicare Part B international drug price index pilot scheduled for January 1, 2021. The motion was filed on December 10 and the government filed its opposition today.
A friend of the FEHBlog pointed out this NIH press release on the state of bad teenager habits.
Findings released today from the most recent Monitoring the Future (MTF) survey of substance use behaviors and related attitudes among teens in the United States indicate that levels of nicotine and marijuana vaping did not increase from 2019 to early 2020, although they remain high. The annual MTF survey is conducted by the University of Michigan’s Institute for Social Research, Ann Arbor, and is funded by the National Institute on Drug Abuse (NIDA), part of the National Institutes of Health.
In the four years since the survey began including questions on nicotine and marijuana vaping, use of these substances among teens have increased to markedly high levels From 2017 to 2019, the percentage of teenagers who said they vaped nicotine in the past 12 months roughly doubled for eighth graders from 7.5% to 16.5%, for 10th graders from 15.8% to 30.7%, and for 12th graders from 18.8% to 35.3%. In 2020, the rates held steady at a respective 16.6%, 30.7%, and 34.5%. However, somewhat encouragingly, daily, or near daily (20 occasions in the past 30 days), nicotine vaping declined among 10th and 12th graders from 2019 to 2020, by close to half — from 6.8% to 3.6% in 10th grade and from 11.6% to 5.3% in 12th grade.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.