Monday Roundup

The Food and Drug Administration (“FDA”) announced today that the agency has “approved Aduhelm (aducanumab) for the treatment of Alzheimer’s, a debilitating disease affecting 6.2 million Americans. Aduhelm was approved using the accelerated approval pathway, which can be used for a drug for a serious or life-threatening illness that provides a meaningful therapeutic advantage over existing treatments. Accelerated approval can be based on the drug’s effect on a surrogate endpoint that is reasonably likely to predict a clinical benefit to patients, with a required post-approval trial to verify that the drug provides the expected clinical benefit.
“Under the accelerated approval provisions, which provide patients suffering from the disease earlier access to the treatment, the FDA is requiring the company, Biogen, to conduct a new randomized, controlled clinical trial to verify the drug’s clinical benefit. If the trial fails to verify clinical benefit, the FDA may initiate proceedings to withdraw approval of the drug.”
The Wall Street Journal adds
Biogen priced the newly approved drug higher than analysts expected. The company said it would charge about $56,000 a year per patient.
A preliminary analysis conducted by the Institute for Clinical and Economic Review, a nonprofit research and advisory group, said the drug could be cost-effective at a per-patient price of $2,500 to $8,300 a year.
Alzheimer’s is a progressive degenerative disease that slowly robs people of their memory and the ability to care for themselves.
About six million people suffer from Alzheimer’s in the U.S. Of those, as many as 1.4 million could be eligible to take Aduhelm, according to estimates by Cigna.
What’s more, according to the Journal,
Cigna will likely cover the drug for people who match the patients studied in Biogen’s clinical trials—those with early-stage Alzheimer’s and amyloid buildup in their brains—said Steve Miller, Cigna’s chief clinical officer.
Most Alzheimer’s patients are covered by Medicare, and their out-of-pocket costs could be significant, depending on their coverage, because of so-called coinsurance payments that require patients to cover a percentage of certain health costs, Dr. Miller said.
“The out-of-pocket testing costs could be a real barrier for those patients who lack the financial means,” said Dr. Miller.
Cigna estimates that patients with traditional Medicare insurance could be on the hook for more than $10,000 a year in coinsurance and copayments for the drug and amyloid testing, Dr. Miller said. Additional costs for people with supplemental Medigap insurance or commercial coverage through Medicare Advantage could reach up to $4,000 annually.
Dr. Miller said patients may be eligible for financial assistance to cover the extra costs through nonprofit foundations, which are often funded by drugmakers.
Healthcare Dive offers a comprehensive article about the new drug that is not behind a paywall.
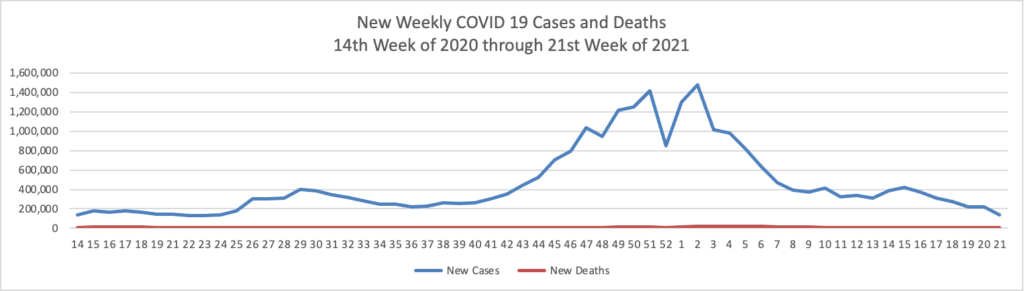
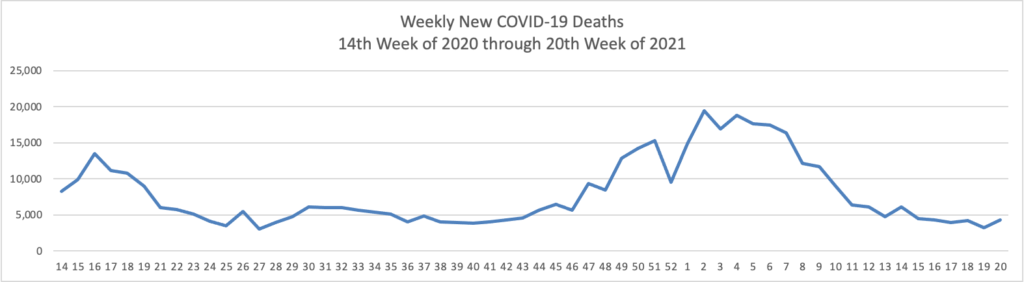
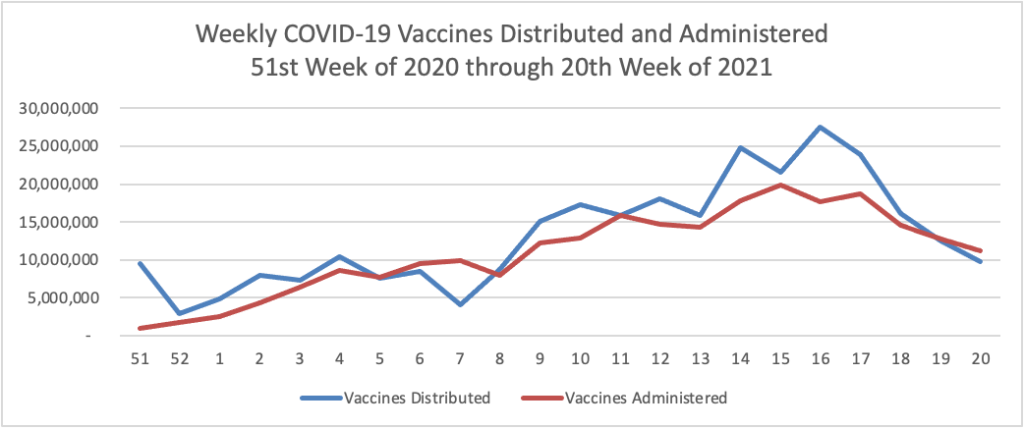
From the COVID-19 front
- David Leonhardt in the New York Times reports on his takeaways from Britain’s recent, modest rise in new COVID-19 cases:
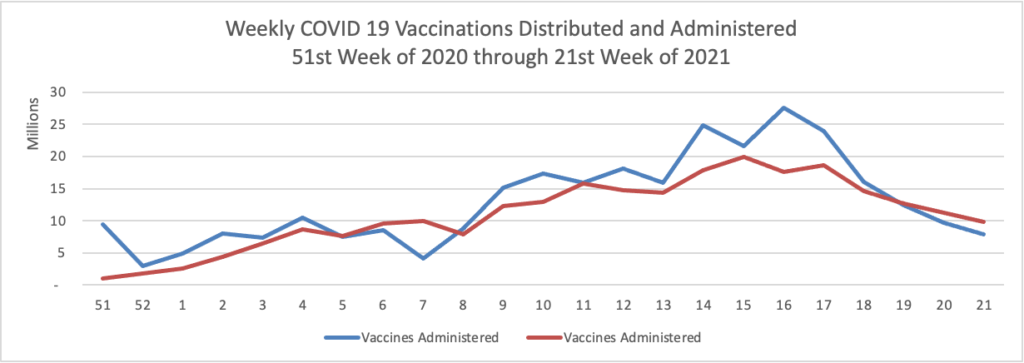
One, vaccines are still the most effective way, by far, to defeat this terrible pandemic. Nothing matters more than the speed at which shots go into arms — in Britain, in the U.S. and especially in poorer countries, where vaccination rates are still low.
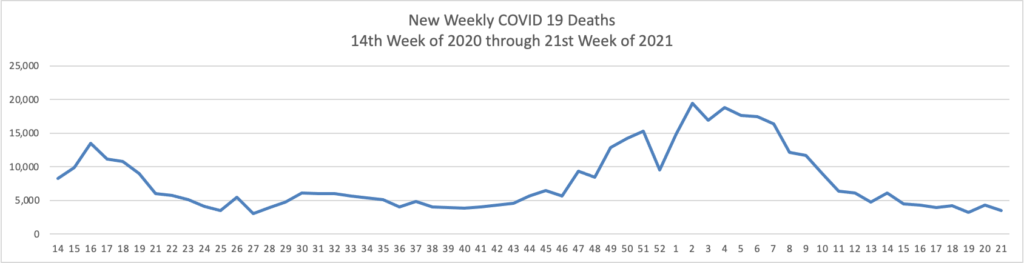
Two, behavior restrictions can still play a role in the interim. If hospitalizations or deaths in Britain rise over the next two weeks, there will be a strong argument for pushing back the full reopening of activities. And that has obvious implications for the U.S., too. Restricting indoor activities for unvaccinated people is particularly important.
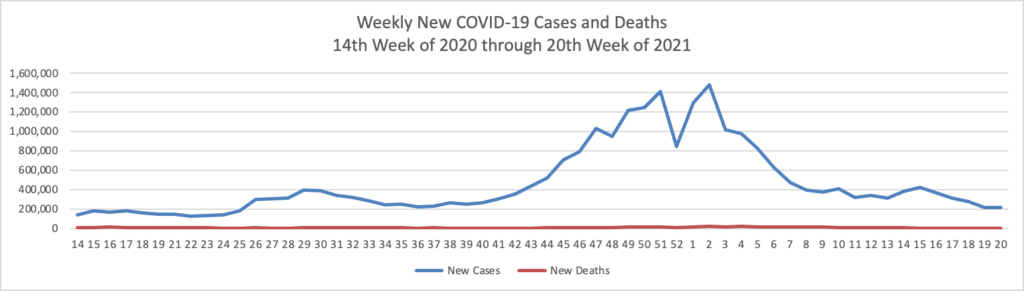
Three, caseloads are no longer as important a measure as they used to be. Before the vaccines were available, more cases inevitably meant more hospitalizations and deaths. Now, the connection is more uncertain. As a recent Times story put it, paraphrasing British scientists, “upticks in new infections are tolerable so long as the vast majority do not lead to serious illness or death.”
- The Society for Human Resource Management discusses stepped-up employer efforts to encourage COVID-19 vaccinations and reduce employee tensions over COVID-19 masks and vaccination in the workplace.
- Medscape offers suggestions for healthcare providers and possible health plans on how to target COVID-19 vaccine hesitancy.
- The Massachusetts Institute of Technology’s Pandemic Technology Project reports on best community practices in closing COVID-19 vaccination gaps.
From the OPM front
- Govexec informs us that OPM “on Monday moved to finalize new regulations making it easier for federal agencies to bring back former employees at a higher salary than when they left government. Currently, federal agencies have the authority to rehire former federal workers outside the competitive hiring process, but they can only offer them positions at the same pay grade they held before they left federal service. Under a final rule set to be published in the Federal Register Tuesday, effective July 8, agencies will be able to use that process to rehire former federal workers at higher salaries than when they left government, accounting for the experience and skills they gained through education and the private sector.”
- Federal News Network informs us that “Federal retirement activity slowed across the board last month, from new claims to backlogged cases and even the time it takes to process them. The latest numbers from the Office of Personnel Management showed that 7,684 new claims were filed in May compared to 9,414 in April — an 18.4% decrease month over month but a 15.6% increase from the same time a year ago. The number of claims processed also dropped to 8,451 in May versus 11,396. That’s a 25.8% decline month other month, although April was unusually high for processed claims when compared to historical monthly totals. May’s processed claims were about even year over year. The retirement backlog decreased from 25,386 claims in April to 24,619 claims in May, but that represented a 35.4% increase from May 2020. In January of this year, the backlog, which has not met it’s goal of 13,000 claims for more than a year and a half, peaked at 26,968 claims and has slowly inched back down.” It’s the FEHBlog’s understanding that OPM’s issues stem from an unnecessarily complex federal retirement system that only Congress can fix.
In other news
- Beckers Hospital Review reports that “Walmart Health’s primary care medical group has filed paperwork to expand virtual care in 16 more states, Insider reported June 7.”
- Healthcare Dive informs us that even before the new information blocking rule’s effective date, “the majority of hospitals have allowed patients to view and download their health information via their own patient portal [in recent year] . However, hospitals allowing patients to use third-party apps to see their data increased sharply from 2018 to 2019, according to a new report from the federal agency that regulates U.S. health IT.”