Thanks to Alexandr Hovhannisyan for sharing their work on Unsplash.
This week, the House of Representatives and the Senate will be in session for flooring voting and Committee business. In addition, the House and the Senate will be taking District and State work breaks for two weeks beginning next Monday.
From the Omnicron and siblings front, the New York Times Well column advises on preparing now for the next surge. Of course, as we lawyers say, the Times is assuming facts not in evidence. Nevertheless, given the huge Omnicron surge last winter, an ounce of prevention may become a pound of cure.
Last week, Bloomberg updated its Covid resiliency ranking of the world’s countries. The U.S ranks 24. Norway, the United Arab Emirates, and Ireland hold the top three spots. Mainland China ranks 48, and Russia and Hong Kong have the last two spots, 52 and 53.
Mark Cuban’s drug company started with an ambitious premise: to circumvent middlemen to offer cheaper costs to patients.
To do so, the company has had to grapple with which parts of the supply chain to develop themselves, and which to outsource using unusually transparent contracts, Mark Cuban Cost Plus Drug Company Founder and CEO Alex Oshmyansky said Thursday at STAT’s Breakthrough Science Summit.
“We decided that the only way to really ensure that pricing for our products actually reaches the patient, the most important part at the end of the day, was to build essentially a parallel supply chain,” Oshmyansky said.
But the company’s ambitions to entirely recreate the pharmaceutical supply chain have started smaller in the process of exploring what’s possible, and what’s profitable.
For example, instead of manufacturing many drugs to sell them cheaply, the company is choosing to focus on manufacturing drugs in shortage to ensure there’s a market for them, and working directly with existing generic manufacturers to keep costs down.
“We basically said, ‘Hey, why don’t we, instead of going through the effort of manufacturing these products ourselves, why don’t we just purchase them and just sell them close to their actual price?’” Oshmyansky said.
A lofty plan to create their own pharmacy benefit manager has also been shelved for the moment, though Oshmyansky insisted it’s not off the table entirely. Instead of creating its own PBM, the company instead chose to whitelist PBMs that behave well for the moment.
From the health plan front —
OPM and AHIP will hold the annual FEHB Carrier Conference later this month. Recently AHIP posted the conference agenda. In addition, the early registration discount ends on Friday, April 8.
Last week, AHIP provided a lengthy list of health insurer actions to address social determinants of health. Bravo.
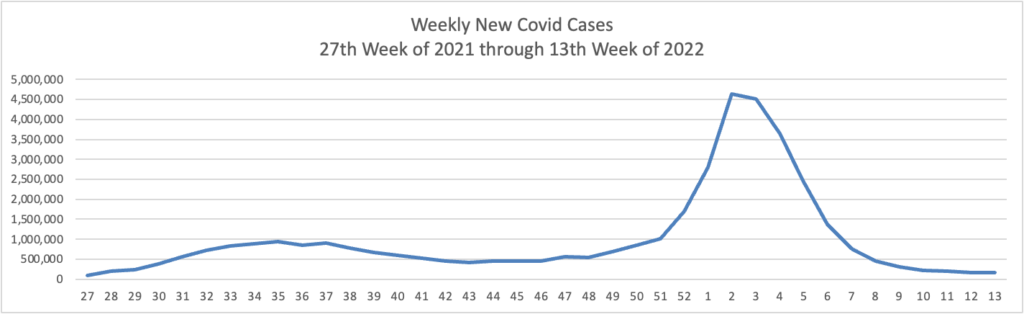
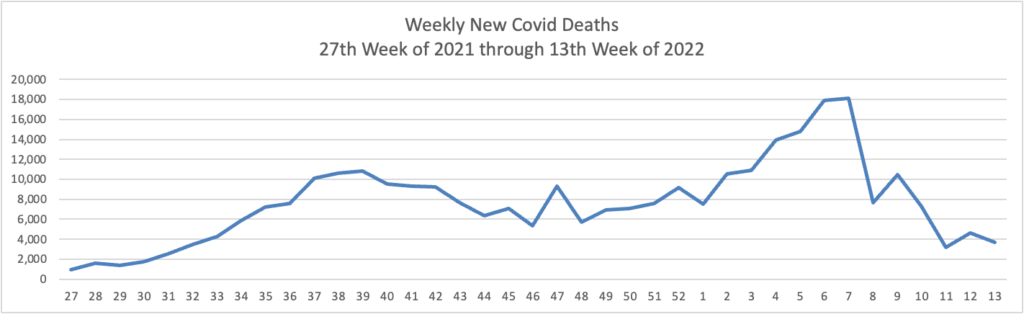
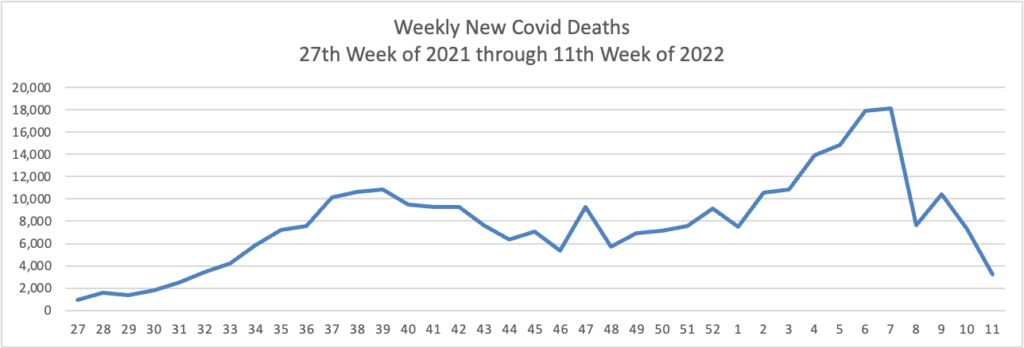
Based on the Centers for Disease Control’s Covid data tracker and using Thursday as the first day of the week, here are the FEHBlog weekly charts of new Covid cases and deaths from the 27th week of 2021 through the 13th week of 2022:
Currently, there are 19 (0.59%) counties with a high COVID-19 Community Level, 146 (4.53%) counties with a medium Community Level, and 3,059 (94.88%) counties with a low Community Level. This represents a slight (−0.84%) decrease in the number of high-level counties, a moderate (−2.73%) decrease in the number of medium-level counties, and a corresponding (+3.57%) increase in the number of low-level counties. Twenty-seven (48.21%) of 56 jurisdictions had no high- or medium-level counties this week. To check your COVID-19 community level, visit COVID Data Tracker.
* * *
The current 7-day daily average [of new Covid hospital admissions] for March 23–29, 2022, was 1,564. This is a 15.8% decrease from the prior 7-day average (1,858) from March 16–22, 2022. * * *
The current 7-day moving average of new [Covid] deaths (627) has decreased 14.4% compared with the previous 7-day moving average (732).
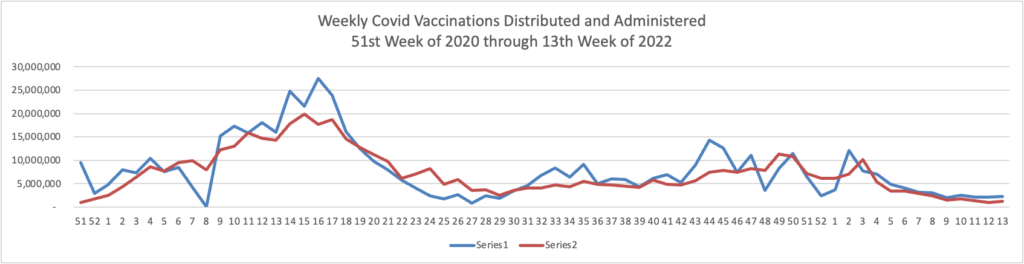
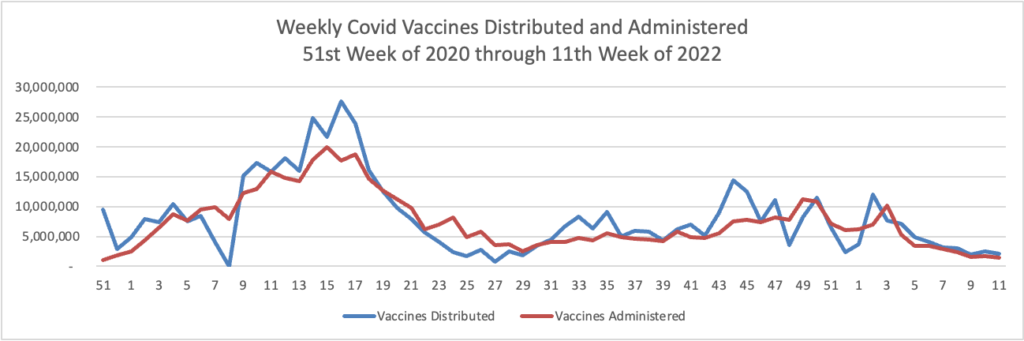
Here’s a link to the FEHBlog’s weekly chart of new Covid vaccinations distributed and administered from the beginning of the Covid vaccination era until last Wednesday.
CDC’s COVID Data Tracker displays vaccination trends by age group, race/ethnicity, and urban/rural status. To see trends by age group and race/ethnicity, visit the Vaccination Demographic Trends tab. To see trends by urban/rural status, visit the COVID-19 Vaccination Equity tab.
The American Medical Association offers guidance to physicians concerning the FDA’s emergency authorization of a second Covid booster for Americans aged 50 and older.
HR Dive discusses what employers should take away from the Biden Administration’s updated approach to Omicron.
Here’s a link to the CDC’s weekly flu surveillance report or Fluview.
From the “and more” department —
HR Dive discusses what employers can do to help employees with adolescent children suffering from behavioral health issues. For example, because a shortage of child psychiatrists exists,
Telemental health programs offer convenient access (often at lower cost than in-person care) for many services—and some, like Brightline, are designed specifically for families of children with mental health needs. However, recent studies have shown that telehealth offerings are not being utilized as much for children as they are for adults, for rural populations as they are for urban ones, or for low-income communities as they are for wealthier ones. Clearly, there is an opportunity for employers to make vulnerable populations aware of the telemental health services available to them.
BioPharma Dive identifies “Five FDA decisions to watch in the second quarter. Between April and June, the agency will advance key regulatory reviews in ALS and gene therapy as well as host an advisory meeting on cancer drugs.”
Health Payer Intelligence tells us about a study, published in JAMA Network Open, finding that insurance “Coverage mandates for a certain kind of breast cancer screening known as DBT may drive utilization upward and cost downward, but the value of this screening remains uncertain.” The article notes “there are steps payers can take [now] to improve cancer patient navigation and patient experience, including reforming network adequacy and streamlining appeals processes.”
Here is a link to OPM’s 2023 Congressional Budget Justification for Fiscal Year 2023, which confirms on page 36
Beginning in plan year 2023, this proposal would require all plans and issuers, including FEHB carriers, to cover three primary care visits and three behavioral health visits each year without charging a copayment, coinsurance, or deductible-related fee. For High Deductible Health Plans, these services would be considered pre-deductible for meeting Health Savings Account requirements. This proposal would increase FEHB premiums by approximately 0.8 percent.
In the FEHBlog’s opinion, OPM should condition these “free” visits on requiring the plan member to identify and use an in-network primary care provider or in-network primary behavioral care provider. Members who develop relationships with their healthcare providers in this manner are more likely to undergo preventive care and otherwise follow medical advice. That’s common sense. It’s worth adding that the Affordable Care Act typically limits reduced cost-sharing to claims involving in-network care.
Meanwhile, Meritalk discusses OPM’s perspective on the President’s proposed budget, and Federal News Network explains why diversity goals are crucial to the success of OPM’s FY 2022 to FY 2026 strategic plan.
FedSmith.com discusses the impact of retirement on federal employee benefits.
From the Omicron (and siblings) front, the Wall Street Journal reports
President Biden on Wednesday said the nation was in a new phase of the Covid-19 pandemic as he marked the launch of a new federal website where Americans can identify virus risks in their areas and recommendations for mitigating the threat.
“We’re now in a new moment in this pandemic,” Mr. Biden said. “It does not mean that Covid-19 is over. It means that Covid-19 no longer controls our lives.”
The FEHBlog is pleased to see that the new site includes a link that allows you to find a test to treat program near you.
From the Rx coverage front, BioPharma Dive informs us
By a slim margin, advisers to the Food and Drug Administration have concluded that the agency should hold off approving a closely watched, experimental medicine for ALS until researchers generate more evidence that it works.
Composed of neuroscience and drug development experts, the 10-person advisory committee on Wednesday voted 6 to 4 against the medicine, named AMX0035 and developed by the Cambridge, Massachusetts-based biotechnology company Amylyx Pharmaceuticals. In a study of about 140 volunteers, AMX0035 appeared to show modest benefits on survival and day-to-day function for patients with rapidly progressing ALS, better known to some as amyotrophic lateral sclerosis or Lou Gehrig’s disease. * * *
The FDA isn’t required to follow its advisers’ recommendations. But it usually does, making approval of AMX0035 now more of a long shot. A final decision is expected by late June.
In other news —
RAC Monitor notes that the Consolidated Appropriations Act 2022 continues to prohibit federal funding for the national patient identifier otherwise required by HIPAA. That’s unfortunate for the country.
Healthcare Economist discusses its views on high deductible plans that are a prerequisite to funding health savings accounts.
The President released his Administration’s fiscal year 2023 proposed budget today. Here are links to OMB’s budget website and a Roll Call overview of the proposal.
Amend administration of tribal FEHB enrollment system
Expand family member eligibility under FEDVIP (presumably increasing the age limit for eligible children from 22 to 26)
Expand FEDVIP to tribal employees
Expand FEHB to tribal colleges and universities.
OPM also released the agency’s FY 2022 to FY 2026 strategic plan today. Here is a link to OPM’s lookbook on that plan. The lookbook (p. 9) identifies one current agency priority goal related to the FEHBP (out of six in total)
Improve customer experience by making it easier for Federal employees, annuitants, and other eligible persons to make more informed health insurance plan selection. By September 30, 2023, complete user-centered design and develop a minimum viable product for a new, state-of-the-art FEHBP Decision Support Tool that will give eligible individuals the necessary information to compare plan benefits, provider networks, prescription costs, and other health information important to them and their families.
In other government reports, the Centers for Medicare and Medicaid Services issued
the 2021-2030 National Health Expenditure (NHE) report, prepared by the CMS Office of the Actuary, that presents health spending and enrollment projections for the coming decade. The report notably shows that despite the increased demand for patient care in 2021, the growth in national health spending is estimated to have slowed to 4.2%, from 9.7% in 2020, as supplemental funding for public health activity and other federal programs, specifically those associated with the COVID-19 pandemic, declined significantly.
From the Omicron and siblings front —
The Centers for Disease Control posted a new “Quarantine and Isolation Calculator — A tool to help determine how long you need to isolate, quarantine, or take other steps to prevent spreading COVID-19.”
The Institute for Clinicial and Economic Review issued an evidence report on four Covid outpatient treatments, including the Pfizer and Merck Covid pills.
ICER’s evidence ratings for the treatments reviewed include:
Sotrovimab delivers at least a small net health benefit when compared to no active treatment, with the possibility of a substantial net health benefit (“B+”).
[Merck’s] Molnupiravir is at least comparable to no active treatment, with the potential of a small net health benefit (“C+”).
[Pfizer’s] Paxlovid delivers at least a small net health benefit when compared to no active treatment, with the possibility of a substantial net health benefit (“B+”).
Fluvoxamine is at least comparable to no active treatment, with the potential of a small net health benefit (“C+”).
From the health equity front, Health Leaders Media reports
Despite willingness to address social drivers of health, two-thirds of physicians report inadequate time or ability to act, according to a new survey report.
KEY TAKEAWAYS
Nearly all physicians reported that at least one social driver of health affected the health outcomes of all or some their patients.
Financial instability (34% of patients) and transportation problems (24% of patients) were the top two social drivers of health experienced by physicians’ patients.
A solid majority of physicians (80%) reported that addressing social drivers of health is essential to improve health outcomes and decrease healthcare costs.
From the Rx coverage front, the FEHBlog noticed today that GoodRx has added a telehealth option to its website.
The President will send his fiscal year 2023 federal budget to Capitol Hill tomorrow. The Wall Street Journal offers an explanatory article about this process.
From the federal employment front, Federal News Network discusses the progress of recalling federal employees to their offices.
Also, the FEHBlog noticed that the Federal Times offers a 2022 Federal Benefits Guide — “Answers to commonly asked questions from federal employees, helpful resources, and more.”
From the vaccines front —
Precision Vaccines informs us “After decades of false starts, new research indicates four Respiratory Syncytial Virus (RSV) vaccine candidates are nearing the completion of late-stage trials. According to the U.S. CDC, RSV vaccines could drastically reduce hospital and intensive-care admissions for young children and seniors.” Fingers crossed.
[T]here is now a growing body of research that’s offering at least some reassurance for those who do end up getting infected — being fully vaccinated seems to substantially cut the risk of later developing the persistent symptoms that characterize long COVID.
While many of the findings are still preliminary, the handful of studies that have emerged in the past half year are telling a relatively consistent story.
“It may not eradicate the symptoms of long COVID, but the protective effect seems to be very strong,” says epidemiology professor Michael Edelstein, of Bar-Ilan University in Israel, who’s studying long COVID.
From the mental healthcare front —
The Wall Street Journal reports “Telemedicine startups make it easier to get ADHD Drugs. That made some [startup] workers anxious. Digital companies such as Cerebral and Done seized on looser pandemic rules for prescribing ADHD drugs like Adderall. Some workers said they felt pressure to provide the medications.”
Employee mental healthcare spending rose, and employer mental healthcare spending fell after employers transitioned their workers from preferred provider organizations to high deductible health plans, a study from the Employee Benefit Research Institute (EBRI) found.
The researchers focused on individuals who had been diagnosed with one of three specific mental health conditions to assess the impact of transitioning from a preferred provider organization to a high-deductible health plan: anxiety, attention deficit hyperactive disorder (ADHD), and major depressive disorder (depression).
The study received funding from a handful of organizations, including the Blue Cross Blue Shield Association, the Independent Colleges and Universities Benefits Association (ICUBA), Pfizer, and PhRMA.
“Smarter deductibles accommodating services preventing the exacerbation of chronic conditions might be a natural evolution of health plans,” the study concluded. “Interventions that improve patient-centered outcomes while maintaining affordability may be found in the form of a clinically nuanced health plan that better meets workers’ clinical and financial needs.”
Because it remains National Kidney Month, the FEHBlog wishes to draw attention to this Fierce Healthcare article about how CVS Health offers personalized kidney care for health plan members.
CVS Kidney Care aims to provide an end-to-end experience to manage kidney care in the long term before it reaches chronic kidney disease or end-stage renal disease. It takes a home-first approach to its care model and is currently co-developing a hemodialysis device that is built specifically with home care in mind.
The device is co-developed by Deka Research & Development and is currently in clinical trials. [CVS Kidney Care President Lisa] Rometty said CVS expects to complete the trial by the end of this year, with anticipated approval and launch sometime in 2023.
CVS chose to get involved in developing the tool, she said, because the company saw an unmet need in the market for a device that’s built from the ground up for in-home dialysis rather than adapted to it. Existing tools are not designed to be easy for a senior patient to understand, for example, Rometty said.
“We did it because we really felt strongly at the time that there wasn’t at the time a device that would meet the unique experience and ease of use and also the safety and clinical aspects,” Rometty said.
Today has been the first day of Spring. But, it is the first day of Fall for my youngest son, who is studying medicine at Queensland University in Brisbane, Australia.
The House of Representatives is on a district work break this week. Meanwhile, the Senate will be engaged in committee business and floor voting on Capitol Hill.
Fedweek discusses the highlights of the call letter for 2023 benefit and rate proposal letters that OPM released last week.
OPM has told FEHB carriers to continue with increased levels of telehealth and other services related to the pandemic in the 2023 plan year, while also either ordering or encouraging them to expand benefits for certain other conditions.
While Fedweek gets the facts right, its article overlooks that OPM’s orders diminish FEHB competition which Congress relies upon to control premiums.
From the cost management front, Fierce Healthcare tells us
While prior authorization is a key tool in an insurer’s arsenal as it thinks about managing costs, the process remains a key source of friction with physicians.
Amid a nationwide conversation around addressing physician burnout and stress, plans are seeking ways to grow automated and virtual prior auth technologies to ease those barriers. At eviCore Healthcare, the benefit management arm of Cigna’s Evernorth subsidiary, the team has found one of the keys to success in this endeavor is bringing physicians into the conversation early on.
Eric Gratias, M.D., eviCore’s chief medical officer, told Fierce Healthcare that prior authorization programs are often built by people who, while well-intentioned, lack first-hand knowledge of what a clinical encounter is like.
The company’s own prior authorization technology, intelliPath, is built on collaboration with physicians who are actively practicing, he said.
“That partnership with our provider clients is absolutely critical for our success,” Gratias said.
Good point.
From the Rx coverage front
NPR Shots points out significant problems with the distribution of Covid treatments.
[D]ata on COVID treatment utilization, shared with NPR by the U.S. Department of Health and Human Services, indicates that millions of COVID treatments are sitting on shelves unused.
“We are still in a public health emergency,” said Dr. Derek Eisnor, who leads the government’s distribution of COVID drugs, on a call with national health organizations on March 16. He urged health leaders to try to get the drugs to communities that have a demand for them, rather than let them go to waste.
“There’s an assumption that there’s not enough of [these drugs] around but it does seem when you look at the numbers that there is a lot around — it’s just not being used,” says Dr. Amesh Adalja, an infectious disease physician and senior scholar at the Johns Hopkins Center for Health Security. “They clearly are not getting to people at high enough rates to have their maximum impact.” * * *
It can be hard to know which pharmacies have the pills in stock or which infusion clinics have appointments available. A patient needs to be able to quickly find a clinician, get a diagnosis and prescription, and be able to access the treatment, all within a few days.
“It’s multifactorial why these drugs are underutilized,” Adalja says. “It’s likely all of those things are playing some role in the discrepancies between what’s been ordered and and what’s actually been administered.”
The Biden administration launched the Test to Treat initiative this month to address these gaps. “We know the challenges that are involved with patients obtaining therapeutics,” said Dr. Meg Sullivan, acting chief medical officer for HHS’ Office of the Assistant Secretary for Preparedness and Response, in a call with clinicians on March 12. The program aims to improve access to rapid testing and to bolster public and provider awareness of available COVID treatments and how to get them.
Here is a link to the HHS website that offers a U.S map that “displays public locations that have received shipments of U.S. Government-procured COVID-19 therapeutics under U.S. Food and Drug Administration (FDA) Emergency Use Authorization (EUA) authority. The long-acting antibody combination, Evusheld; monoclonal antibody treatments, bebtelovimab and sotrovimab; as well as the oral antiviral therapies, Paxlovid and molnupiravir are products authorized by the FDA for either prevention (Evusheld) or treatment (Paxlovid, sotrovimab, bebtelovimab, and molnupiravir) of COVID-19. The locations displayed in the locator have reported available courses within the last seven days.”
The test to treat program’s website is not online yet as far as the FEHBlog can tell.
On March 30, the Food and Drug Administration is bringing together outside experts in neurology to review an experimental drug from Amylyx for the treatment of amyotrophic lateral sclerosis, or ALS. The hearing is expected to be closely watched by ALS patients and their advocates, given the significant need for new treatments for the disease.
But the hearing is likely to garner extra attention because it’s the first meeting of the FDA advisory group since it met in November 2020 and voted unanimously against the approval of Aduhelm, Biogen’s drug for Alzheimer’s disease. The FDA later ignored that recommendation and approved the medication, leading to the resignation of three members of the panel and an uproar over whether the agency had compromised its standards.
Sixteen months removed from all the Aduhelm drama, the Peripheral and Central Nervous System (PCNS) Drugs Advisory Committee, restocked with new members, is back to tackle another high-stakes review of a drug targeting a progressive, fatal nervous system disease. The Amylyx treatment — called AMX0035 — isn’t likely to generate the same acrimony as Aduhelm, but it could similarly force the FDA to bend its standards.
Here’s what you need to know about AMX0035, the data from its single clinical trial, and the issues that are likely to take center stage at the FDA advisory panel meeting.
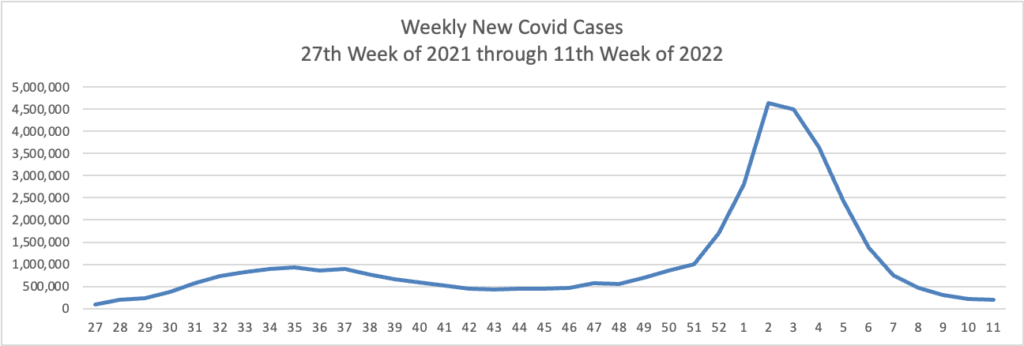
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s latest weekly charts of new Covid cases and deaths (a lagging indicator):
The CDC observes in its weekly review of its Covid statistics
COVID-19 cases, hospitalizations, and deaths all continue to decrease in the United States. According to CDC’s COVID Data Tracker, as of March 16, 2022, 76.7% of the total U.S. population has received at least one dose of a COVID-19 vaccine, and 65.3% has completed their primary series. However, only about half of the booster-eligible population has received a booster dose and is considered up to date on their COVID-19 vaccines.
Two new studies show the effectiveness of COVID-19 vaccines and boosters across periods of three variants of concern (Alpha, Delta, and Omicron). CDC released a study today showing that, among adults hospitalized with COVID-19 during the Delta and Omicron waves, those who received two or three doses of the Pfizer-BioNTech or Moderna vaccine had 90–95% less risk of dying or needing a ventilator compared with adults who were not vaccinated. Protection was highest in adults who received a third COVID-19 vaccine dose. A study published in the British Medical Journalexternal icon found that vaccines gave a high level of protection against hospitalization for all variants, but not as much for Omicron among adults who received only a primary series. However, boosters increased protection against Omicron. The study also showed that hospital patients who were vaccinated had much lower disease severity than patients who were not vaccinated.
These studies emphasize the importance of staying up to date with vaccinations—they are our best protection against severe COVID-19 illness. Vaccination is also the safest way to reduce the chance that new variants will emerge. Find a vaccine provider and get your booster dose as soon as you can.
In that regard, here is the FEHBlog weekly chart of Covid vaccinations distributed and administered from the beginning of the vaccination era in late 2020:
Here’s a link to the Food and Drug Administration’s March 18 round of its Covid related activities.
While the bulk of Covid care spending goes to hospitals, Becker’s Hospital Review reports that a “sizable minority” have a significant amount out-of-pocket spending for this care, according to a study published in the American Journal of Managed Care March 16.”
It’s worth adding that the Wall Street Journal reports that
The biggest credit-reporting firms will strip tens of billions of dollars in medical debt from consumers’ credit reports, erasing a black mark that makes it harder for millions of Americans to borrow.
Equifax Inc., ExperianPLC and TransUnion are making broad changes to how they report medical debt beginning this summer. The changes, which have been in the works for several months, will remove nearly 70% of medical debt in collections accounts from credit reports.
Beginning in July, the companies will remove medical debt that was paid after it was sent to collections. These debts can stick around on a consumer’s credit report for up to seven years, even if they are paid off. New unpaid medical debts won’t get added to credit reports for a full year after being sent to collections.
The firms are also planning to remove unpaid medical debts of less than $500 in the first half of next year. That threshold could rise, according to people familiar with the matter.
From the compliance front —
The Internal Revenue Services issued a notice on how to calculate the No Surprises Act’s Qualified Payment Amount when the health plan does not have enough data to calculate a January 2019 median.
The Department of Labor is offering a webinar on March 30 at 11 am that “will help employers, service providers, and benefit professionals understand how the provisions of [the federal mental health partity act] apply to employer-sponsored group health plans and provide information on how to avoid common problems. The webinar runs about 45 minutes to an hour and is limited to 200 participants.
From this week’s healthcare conferences front
Fierce Healthcare discusses the electronic medical records interoperability theme of the HIMSS conference.
Fierce Healthcare also offers a wrap report on “the most interesting innovations at SXSW 2022: From holograms to the future of psychedelics.”
From the telehealth front
Becker’s Payer Issues reports that most consumer driven plans have taken advantage of the IRS offered flexibility to cover telehealth before the “high” annnual deductible.
Forbes informs us “Telehealth Accounts For One In Three Mental Health Visits Two Years Into Pandemic.” Whoopee.
From the good works department, the American Medical Association tells us about a North Carolina physician who is talking the diabetes problem.
Dr. [Brian] Klausner is the medical director of WakeMed’s Community Population Health program in Raleigh. He also is a physician champion for DiabetesFreeNC. That is the statewide initiative where AMA partnered with the North Carolina Medical Society and others to support collaborative efforts to end type 2 diabetes in the Tar Heel State.
Rather than think of the pandemic as having “derailed” diabetes prevention or other population health efforts, Dr. Klausner said that “COVID-19 expedited new perspective in how we can do a better job addressing historic roadblocks to community health initiatives, including those related to diabetes and prevention.”
Happy Ides of March. The President signed the Consolidated Appropriations Act 2022 into law today. The Postal Reform Act of 2022 continues to await the President’s signature.
From the Omicron front, David Leonhardt reports on COVID surges in China and Europe. He concludes
Even if [Covid] cases rise [in the U.S. again], as seems likely, there are good reasons not to panic. Vaccination tends to turn Covid into a mild illness, especially for people who have received a booster. For the unvaccinated and unboosted, BA.2 is another reason to get a shot.
It’s also a reason for the federal government and states to expand access to both Evusheld — a drug that can help protect the immunocompromised — and Paxlovid — a post-infection treatment. Finding either is often difficult today. (If you’re looking for one of them, click on this link for Evusheld and this one for Paxlovid.)
The bottom line: Covid isn’t going away, but vaccination and other treatments can keep future increases manageable. The biggest problem remains the millions of people who remain unvaccinated, many of them by choice. That’s the case in the U.S., in Hong Kong and across much of Europe, Africa and the rest of the world.
Inducing more people to get shots — through persuasion or mandates — would probably save more lives than any other Covid policy.
What is the FDA’s hold up in reviewing the standard Covid vaccines for which emergency use authorizations have been filed? As previously noted, the traditional vaccines may be appealing to those resistant to the state-of-the-art mRNA vaccines.
The Wall Street Journal reports
Pfizer Inc. and partner BioNTech SE have asked U.S. health regulators to authorize a second booster dose of its Covid-19 vaccine for people 65 years and older.
The companies said Tuesday that they had filed the application. The Food and Drug Administration is expected to make a decision in time for the Biden administration to begin a potential fall vaccine campaign.
The FDA has been reviewing data and looking at potentially authorizing a fourth dose of the shot for use in the fall, The Wall Street Journal reported last month.
From the Rx coverage front —
STAT News informs us
The prices pharmacy benefit managers and insurers pay for Sanofi medicines have decreased for a sixth consecutive year, yet patient out-of-pocket costs are rising. Once again, there is further evidence that focusing solely on lowering the list price of medicines doesn’t guarantee lower costs for patients. Sanofi pulls back the curtain on the impact of list and net prices and more in its annual pricing report.
and
Back in 2019, when the Senate Finance Committee called seven drug industry CEOs to testify, it seemed like proof that Washington was within striking distance of actually reining in the industry’s high prices. “It’s past time to get beyond the excuses and make prescription drugs affordable,” Sen. Ron Wyden, the top Democrat on the committee, told drugmakers that day. Tomorrow, almost exactly three years later, Wyden will chair another hearing on prescription drug pricing. He’s billing the hearing as “an opportunity for members to discuss how high drug prices have impacted seniors and families in their states and identify solutions” — even though lawmakers have had more than a dozen such hearings to “discuss” high drug prices over the past three years. STAT’s Nicholas Florko tallies what’s at stake in STAT+.
In FDA News, the agency reports approving today “the first generic of Symbicort (budesonide and formoterol fumarate dihydrate) Inhalation Aerosol for the treatment of two common pulmonary health conditions: asthma in patients six years of age and older; and the maintenance treatment of airflow obstruction and reducing exacerbations for patients with chronic obstructive pulmonary disease (COPD), including chronic bronchitis and/or emphysema. This complex generic drug-device combination product, which is a metered-dose inhaler, should not be used to treat acute asthma attacks.”
From the opioid epidemic front, “the Department of Health and Human Services (HHS), through the Substance Abuse and Mental Health Services Administration (SAMHSA), announced two grant programs totaling $25.6 million that will expand access to medication-assisted treatment for opioid use disorder and prevent the misuse of prescription drugs. By reducing barriers to accessing the most effective, evidence-based treatments, this funding reflects the priorities of HHS’ Overdose Prevention Strategy, as well as its new initiative to strengthen the nation’s mental health and crisis care systems.”
From the patient front, HHS’s Agency for Healthcare Research and Quality announced the agency’s
Support for Patient Safety Awareness Week. Ongoing investments in safety research, the development of safety toolkits and training resources, and a growing emphasis on improving diagnostic safety are all part of a mission to make healthcare safe for all Americans. Access more information about AHRQ’s support of Patient Safety Awareness Week, including a special introductory video from Jeff Brady, M.D., director of the Center for Quality Improvement and Patient Safety; information about how to get involved in Patient Safety Awareness Week activities; and recent patient and diagnostic safety resources, including:
The Biden administration has been working on additional rulemaking to address issues with the payer-to-payer data exchange requirements set out in sweeping interoperability rules finalized in early 2020, and “we look forward to sharing this rule with you soon,” CMS administrator Chiquita Brooks-LaSure told attendees at the HIMSS annual conference in Orlando on Tuesday.
CMS decided not to enforce those provisions when they kicked in this year, after health insurers raised concerns about operational challenges and risks to data quality given a lack of specificity in the rule.
The new rule will incorporate extensive public comment to try to address stakeholder concerns, and will standardize how payers exchange data through application programming interfaces, Brooks-LaSure said.
An online tool that allows patients in markets across the country to compare prices for hundreds of hospital services before getting treatment has launched in its beta development stage.
Turquoise Health’s platform uses cost data from machine-readable files made public by hospitals as part of compliance with a federal price transparency rule that went into effect in January 2021.
The San Diego-based startup’s platform includes a scorecard that lets users assess price transparency compliance with the CMS requirements for nearly 6,000 hospitals, Turquoise Health said Monday. Hospitals receive a score based on an algorithm-driven five-star rating system.
Fierce Healthcare reports from the SXSW Conference in Austin, TX.
A new Covid-19 pill from Merck & Co. and Ridgeback Biotherapeutics LP has been more widely used than expected since rolling out late last year, though regulators and many doctors consider it a last resort.
Many doctors and health officials anticipated a rival pill, Pfizer Inc.’s Paxlovid, would be the Covid-19 drug of choice. Paxlovid was found to be far more effective than Merck-Ridgeback’s molnupiravir in clinical trials, and regulators and guidelines recommended using Paxlovid if possible.
Prescriptions for the two antivirals have been running about equal since their authorization in December, however. The larger-than-expected use is a sign of the high demand for easy-to-use coronavirus treatments that can be taken at home, especially during surges like the recent Omicron wave.
Federal agencies are not restricted on the size of events they host, unless under certain conditions, according to new guidelines.
The Biden administration’s Safer Federal Workforce Task Force issued updated and new guidance on March 11, most of which reflects the Centers for Disease Control and Prevention’s new framework released in late February. That framework “moves beyond just looking at cases and test positivity to evaluate factors that reflect the severity of disease, including hospitalizations and hospital capacity, and helps to determine whether the level of COVID-19 and severe disease are low, medium, or high in a community,” as CDC Director Dr. Rochelle Walensky said on a briefing call.
There are no “restrictions on the size of agency-hosted in-person meetings, events, or conferences,” said one of the new “frequently asked question” prompts. “Should an agency intend to host a meeting, conference, or event that will be attended in-person by more than 50 participants at a facility in a county where the COVID-19 Community Level is HIGH, the agency should first seek the approval of its agency head or official to which this responsibility has been delegated, in consultation with the agency’s COVID-19 coordination team.”
The Food and Drug Administration has approved AstraZeneca and Merck & Co.’s drug Lynparza for people with a genetic form of early breast cancer, a decision that could spur greater use of DNA testing in diagnosing and treating the disease.
Lynparza is already used to treat metastatic breast cancer in patients with so-called BRCA gene mutations. The new approval makes Lynparza available earlier in their disease, after surgery to remove a tumor and standard drugs like chemotherapy and radiation. People with cancers that are “HER2-negative” and at a high risk of relapsing are eligible for treatment.
The decision is based on the results of a large study published last year in The New England Journal of Medicine last year. In it, Lynparza reduced the risk of disease progression or death by 42% versus placebo after a median of 2.5 years of follow-up. Updated results show the drug cut the risk of death by about a third, a finding the companies will detail at a medical meeting on Wednesday.
The National Institutes of Health announced launching “a Phase 1 clinical trial evaluating three experimental HIV vaccines based on a messenger RNA (mRNA) platform—a technology used in several approved COVID-19 vaccines.” mRNA developers were working on HIV vaccines before the pandemic struck. Fingers crossed.
Sen. Chuck Grassley (R Iowa) is urging the Federal Trade Commission to “find consensus” and vote again to launch a study into the business practices of pharmacy benefit managers, according to a letter he sent to FTC Chairwoman Lina Khan dated March 9.
“PBMs operate with little to no transparency, making it very difficult if not impossible to understand the flow of money in the prescription drug marketplace,” the Republican senator from Iowa said in his letter, nodding to the bipartisan consensus for such an examination.
Grassley urged the commissioners to come up with a more targeted focus for the study and suggested narrowing a review to the impact on consumers and their out of pocket costs.
From the patient safety front, Beckers Hospital Review explains
Staffing shortages are the top threat to patient safety in 2022, according an annual report on patient safety concerns from ECRI, an organization that conducts independent medical device evaluations, published March 14.
Researchers identified the top threats to patient safety by analyzing a wide range of data, including scientific literature, patient safety events or concerns reported to or investigated by ECRI.
Ten top patient safety concerns this year:
1. Staffing shortages
2. COVID-19 effects on healthcare workers’ mental health
3. Bias and racism in addressing patient safety
4. Vaccine coverage gaps and errors
5. Cognitive biases and diagnostic error
6. Nonventilator healthcare-associated pneumonia
7. Human factors in operationalizing telehealth
8. International supply chain disruptions
9. Products subject to emergency use authorization
10. Telemetry monitoring
From the mental healthcare front, the Department of Health and Human Services announced
A new U.S. Department of Health and Human Services (HHS) study published in the American Medical Association’s journal JAMA Pediatrics reports significant increases in the number of children diagnosed with mental health conditions. The study, conducted by the Health Resources and Services Administration (HRSA), finds that between 2016 and 2020, the number of children ages 3-17 years diagnosed with anxiety grew by 29 percent and those with depression by 27 percent. The findings also suggest concerning changes in child and family well-being after the onset of the COVID-19 pandemic.
From Capitol Hill, overnight, the FY 2022 onmnibus appropriations bill language was released. The bill is over twenty one hundred pages long. The American Hospital Association has taken the time to summarize the bill’s healthcare provisions. Federal News Network discusses the bill’s federal workforce provisions. The Wall Street Journal notes
Democratic House leaders said they would remove a contentious $15.6 billion Covid-19 aid provision from the omnibus spending bill to try to get it over the finish line, after angry rank-and-file members rejected clawing back states’ unused coronavirus money to fund the proposal.
The decision to drop the Covid-19 aid was a dramatic setback for both House Speaker Nancy Pelosi (D., Calif.), who negotiated the plan, and President Biden, whose administration originally asked for $22.5 billion for Covid-19 aid and now will get nothing from the bill.
The House of Representative currently is considering the bill and a fourth continuing resolution that would last the four days beyond March 11 that the Senate needs to pass the bill. The House is expected to vote on the bill around 9:15 pm ET. Passage of the bill and the brief continuing resolution is expected.
From the Rx coverage front, Fierce Healthcare informs us
Amazon Pharmacy is partnering with Blue Plans in five states and Prime Therapeutics to tackle the affordability of prescription medications.
The online retail giant’s pharmacy arm is rolling out a prescription discount savings card that’s available to some Blue Plans members.
Integrating this discount card pricing into the shopping experience lets eligible customers compare their co-pay or discount price upfront and then apply purchases for eligible medications to the out-of-pocket maximums and deductibles associated with their insurance plan, according to Nworah Ayogu, M.D., chief medical officer for Amazon Pharmacy. * * *
Eligible plans now include Horizon Blue Cross Blue Shield of New Jersey, Blue Cross Blue Shield of Nebraska, Blue Cross Blue Shield of Alabama, Florida Blue and Blue Cross and Blue Shield of Kansas.
From the miscellany department —
The National Committee for Quality Assurance has created a health equity website.
America’s Health Insurance Plans celebrated International Womens’ Day yesterday with remarks from healthcare leaders on how health plans can improve healthcare for women.
The Centers for Medicare and Medicaid Services issued new guidance for group health plans on submitting a valid documented defense to Medicare overpayment recovery demands.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.