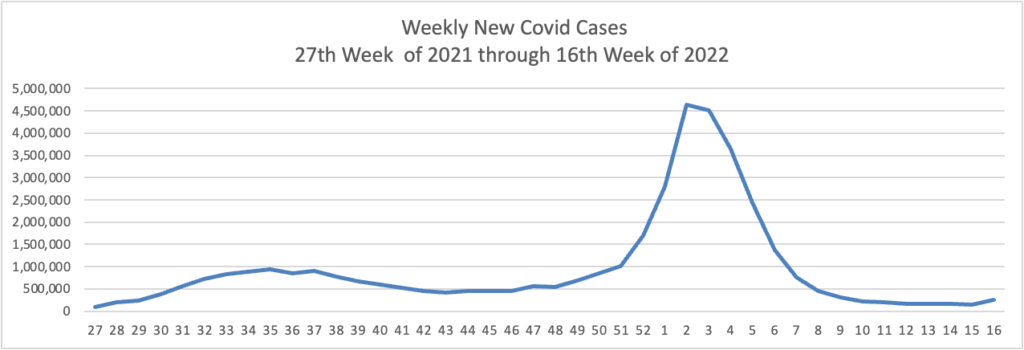
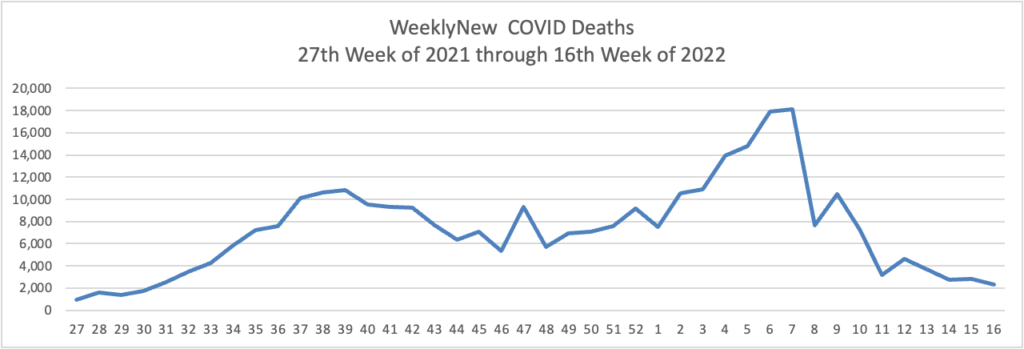
Based on the Centers for Disease Control’s Covid Data Tracker and using Thursday as the first day of the week, here are the FEHBlog’s latest weekly charts of new Covid cases and deaths.
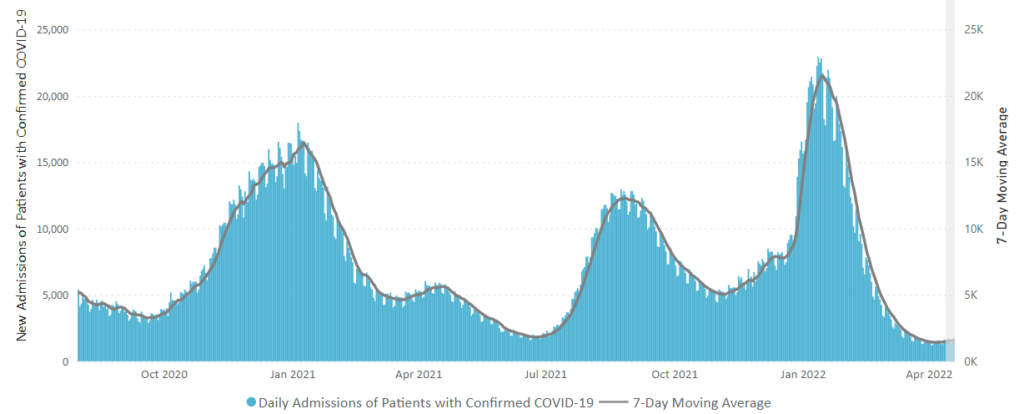
Because David Leonhardt in the New York Times recommends keeping an eye on Covid hospital admissions here is the CDC’s latest chart
The weekly new cases and death chart start in the middle of 2021 when we hit all time lows in new cases. Although our new cases total for the past week was 3 times week 27 in 2021, the new hospitalizations level is lower. That’s good news.
The CDC’s weekly review of its Covid stats adds
Currently, there are 39 (1.21%) counties, districts, or territories with a high COVID-19 Community Level, 231 (7.17%) counties with a medium Community Level, and 2,954 (91.63%) counties with a low Community Level. This represents a slight (0.78%) increase in the number of high-level counties, a small (+1.67%) increase in the number of medium-level counties, and a corresponding (−2.45%) decrease in the number of low-level counties. Twenty-five (44.64%) of 56 jurisdictions had no high- or medium-level counties this week.
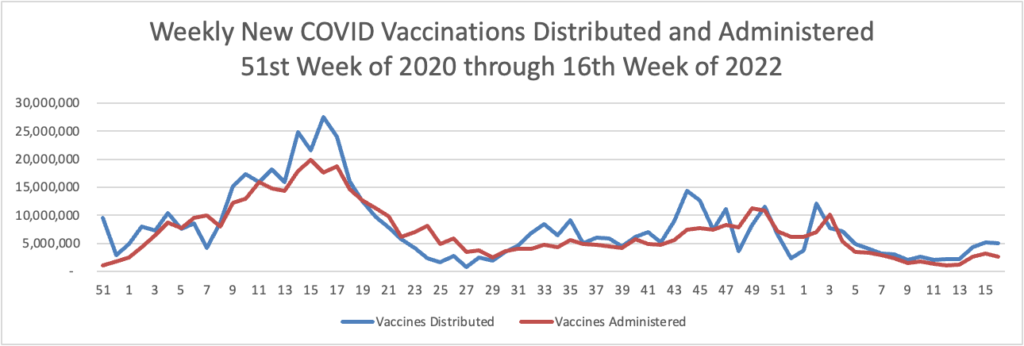
Here’s the FEHBlog’s latest weekly chart of Covid vaccinations distributed and administer from the beginning of the COVID vaccination era to the 16th week of 2022.
New vaccinations remain above 2 million per week.
From the Medicare front, the Centers for Medicare Services announced today a proposed rule that would create five new special Medicare enrollment periods.
An SEP forIndividuals Impacted by an Emergency or Disaster that would allow CMS to provide relief to those beneficiaries who missed an enrollment opportunity because they were impacted by a disaster or other emergency as declared by a Federal, state, or local government entity.
An SEP for Health Plan or Employer Error that would provide relief in instances where an individual can demonstrate that their employer or health plan materially misrepresented information related to enrolling in Medicare timely.
An SEP for Formerly Incarcerated Individuals that would allow individuals to enroll following their release from correctional facilities.
An SEP to Coordinate with Termination of Medicaid Coverage that would allow individuals to enroll after termination of Medicaid eligibility.
An SEP for Other Exceptional Conditions that would, on a case-by-case basis, grant an enrollment period to an individual when circumstances beyond the individual’s control prevented them from enrolling during the IEP, GEP or other SEPs.
These “SEPs that would provide individuals who meet certain exceptional conditions and who missed a Medicare enrollment period an opportunity to enroll without having to wait for the GEP and without being subject to a [Part B] late enrollment penalty.”
UnitedHealth Group subsidiary Optum has quietly acquired at least two independent primary care groups in Oregon, according to The Lund Report.
Optum has purchased Eugene-based Oregon Medical Group and Portland-based GreenField Health. Combined, the two systems have about 120 doctors and clinicians at 11 facilities.
GreenField Health was purchased last year and Oregon Medical Group in late 2020, according to the Lund Report.
Nationwide, UnitedHealth Group has purchased about 1,500 primary care and specialty facilities, totaling 60,000 physicians.
Humana will divest its majority stake in Kindred at Home’s hospice business to investment firm Clayton, Dubilier & Rice.
As part of the deal, which was announced Thursday, Humana will sell off a 60% stake in KAH Hospice for $2.8 billion in cash, which reflects an enterprise valuation of $3.4 billion and twelve times the division’s forecasted earnings before interest, income taxes, depreciation and amortization (EBITDA) for this year.
Humana said a year ago when it bought out the majority stake in Kindred at Home that it planned to divest the hospice arm. The insurer believes that it can deliver strong patient outcomes in hospice care without owning KAH Hospice outright, Chief Financial Officer Susan Diamond said in a statement.
Bay Area biotech Guardant Health is closer than ever to its ultimate goal — developing and deploying a simple, blood-based test that you could get during an annual doctor’s visit to spot cancer early enough that it might be treated more successfully. And 2022 is shaping up to be a big year for the company’s ambitions.
Scientists around the world are discovering and tracking newer forms of the Omicron coronavirus variant, showing how even when a strain becomes globally dominant, it continues to evolve and can splinter into different lineages.
Case in point: Updated data released Tuesday showed that a burgeoning form of Omicron, called BA.2.12.1 — itself a sublineage of the BA.2 branch of Omicron — now accounts for nearly one in five infections in the United States. It’s eating into the prevalence of the ancestral BA.2, highlighting the emergent virus’s transmission advantage over its parent. BA.2 now accounts for about 74% of cases, while the remaining 6% or so are from the BA.1 branch of Omicron, the first form of the variant that took over globally and whose prevalence has been falling as BA.2 became dominant.
The menagerie can be dizzying to track, especially because all these cases technically fall under the Omicron umbrella. But even as scientists closely monitor the divergence of Omicron, early signs suggest the different lineages don’t substantially differ in terms of how virulent they are or in their ability to evade the protection generated by immunizations. While some of the newer forms of the virus might be better spreaders than others, their emergence doesn’t necessarily result in huge increases in cases.
David Leonhardt adds in his New York Times morning column today
In several places where the number of cases has risen in recent weeks, hospitalizations have stayed flat. (In past Covid waves, by contrast, hospitalizations began rising about a week after cases did.) * * *
Even if hospitalizations do rise in coming weeks, a declining share of coronavirus cases that result in serious illness would be very good news, Dr. Craig Spencer, director of global health in emergency medicine at Columbia University, has pointed out.
I haven’t seen a Covid patient in the E.R. in weeks and go to work now expecting not to,” Spencer told me, “despite a swirl of Covid in the community.”
Among other things, a decoupling of cases and severe illness would mean that hospitals were less likely to become overwhelmed during future Covid surges. When hospitals avoid getting swamped, they can provide care to every patient who needs it — which becomes another factor that reduces bad health outcomes.
For these reasons, Mr. Leonhardt plans to shift his focus from new cases to new hospitalizations.
Because mRNA-based vaccines are a relatively new class of vaccines, they do not include the traditional adjuvants. The current mRNA vaccines used in the U.S. rely on small balls of fat called lipid nanoparticles to deliver the mRNA. These lipid molecules can act as adjuvants, but how precisely these molecules affect the long-term immune response remains to be seen. And whether the current COVID-19 vaccines’ failure to trigger strong long-lived antibody response is related to the adjuvants in the existing formulations remains to be explored.
While the current vaccines are highly effective in preventing severe disease, the next phase of vaccine development will need to focus on how to trigger a long-lived antibody response that would last for at least a year, making it likely that COVID-19 vaccines will become an annual shot.
New data from Moderna offer hope that booster shots against Covid-19 could become at least somewhat more effective than they already are. But the data also point to how difficult it could be to determine exactly which Covid shots to give as annual boosters.
At a hearing of a Food and Drug Administration advisory panel earlier this month, experts fretted about exactly how governments should make decisions about the composition of annual boosters. And they were adamant that governments, not pharmaceutical companies, should be deciding the strain composition of the shots, as the World Health Organization does for influenza shots. But these data are a reminder that those decisions can be tough. What would experts do when faced with booster shots with several different compositions? Will adding new strains work similarly for different types of vaccines? There are a huge number of open questions.
There’s also the biggest problem with annual flu shots: People don’t get them. Even with the current Covid boosters, this has been true. Data presented to the FDA panel said that 217 million Americans are vaccinated about Covid. But only 90 million people have received a booster dose. How many will turn out for a new booster next year?
Look at this comparison of winter 2019-2020 flu vs. 2020-2021 Covid
2019 – 2020 Winter CDC Fluview
3/28/20
2020-2021 Winter COVID-19
10/1/2020 to 3/21/2021
Flu Deaths
24,000
COVID-19 Deaths
332,636
Flu Cases
39,000,000
COVID-19 cases
22,399,598
Deaths over total cases
0.06%
1.49%
https://www.cdc.gov/flu/weekly/index.htm
Who would look back on pre-Covid flu as the good old days? But comparatively, it is. We see millions more flu cases, but hundreds of thousands fewer flu deaths.
Kaiser Health News discusses the need for better ventilation in office buildings which could help tamp down Covid and flu cases. “The science is airtight,” said Joseph Allen, director of the Healthy Buildings program at Harvard University’s T.H. Chan School of Public Health. “The evidence is overwhelming.”
From the No Surprises Act front, Healthcare Dive reports
The online portal for resolving payment disputes between payers and providers for certain out-of-network charges is now open, the CMS said Monday. The portal initiates what’s known as the federal independent dispute resolution process, a key part of the No Surprises Act that outlaws balance bills in most cases. As a last resort, it allows payers and providers to resolve payment disputes using an arbitration style similar to the model adopted by Major League Baseball in salary negotiations.
From the transparency in coverage rule front, the Labor Department issued ACA FAQ 53 today. FAQ 53 provides guidance to health plans, including FEHB plans, on how to post three machine-readable pricing files on their website. The Labor Department will begin to enforce this requirement on July 1, 2022.
Commercial health plans pay higher prices than public payers for hospital care, which accounts for more than 5 percent of US gross domestic product. Crafting effective policy responses requires monitoring trends and identifying sources of variation. Relying on data from the Healthcare Provider Cost Reporting Information System, we describe how commercial hospital payment rates changed relative to Medicare rates during 2012–19 and how trends differed by hospital referral region (HRR). We found that average commercial-to-Medicare price ratios were relatively stable, but trends varied substantially across HRRs. Among HRRs with high price ratios in 2012, ratios increased by 38 percentage points in regions in the top quartile of growth and decreased by 38 percentage points in regions in the bottom quartile. Our findings suggest that restraining the growth rate of HRR commercial hospital price ratios to the national average during our sample period would have reduced aggregate spending by $39 billion in 2019.
Seniors save nearly $2,000 on average a year in total healthcare spending in Medicare Advantage (MA) compared to fee-for-service Medicare, a new study finds.
The study, published Tuesday, by the advocacy group Better Medicare Alliance finds that seniors spent $1,965 less including premiums and out-of-pocket costs on MA when compared to fee-for-service.
“We see particularly strong results for historically disadvantaged populations, including Black and Hispanic beneficiaries and those who are low-income,” said Allison Rizer, principal at the consulting firm ATI Advisory, which performed the study that examined 2019 Medicare Current Beneficiary Survey data.
From the healthcare business front, Fierce Healthcare tells us
UnitedHealth Group executives said Thursday that its Optum Health subsidiary, which is one of the country’s largest physician groups, is building out value-based care partnerships at a faster rate than was expected.
In its earnings report, the healthcare giant said it initially projected that 500,000 new patients would be treated in value-based arrangements. It’s upping that projection to 600,000. Wyatt Decker, M.D., CEO of Optum Health, said on the company’s earnings call that reflects Optum’s efforts to invest in technology, analytics and building networks are paying off.
“What you’re really seeing is a result of almost 10 years of building a flywheel that now has significant momentum,” Decker said. “All of that continues to yield benefits and, frankly, growth.”
The severity of multiple sclerosis (MS) was linked with geographic latitude, an observational study showed.
Among 46,000 MS patients living in temperate zones, more severe disease was seen in those who lived above 40° latitude, reported Tomas Kalincik, MD, PhD, of the University of Melbourne, Australia, and co-authors.
The association was driven mainly, but not exclusively, by ultraviolet B (UVB) radiation exposure contributing to both MS susceptibility and severity, the researchers wrote in Neurology.
AHRQ discusses a study on “Geographic Variation in Inpatient Stays for Five Leading Substance Use Disorders, 2016-2018.” There are interesting State variations.
The White House and the U.S. Department of Health and Human Services (HHS) are hosting an upcoming meeting entitled, Conversations on Encouraging COVID-19 Vaccinations, a virtual program that is part of the “We Can Do This” COVID-19 public education campaign.
The virtual Summit will feature conversations among leading doctors, medical professionals, parents, and community leaders about COVID-19 vaccines and how the broader medical community can encourage vaccination among pregnant people, children, teens, and young adults.
Speaking of AHIP, the FEHBlog noticed today that the OPM AHIP FEHB carrier conference website is fully built out. The virtual conference will be held on April 27 and 28.
The Biden administration Monday said it would not enforce the mask mandate for airplanes and transit after a federal judge in Florida struck it down.
In a 59-page order, U.S. District Judge Kathryn Kimball Mizelle said the Centers for Disease Control and Prevention overstepped its authority by requiring passengers to wear masks on public transportation, saying the mandate ”exceeds the CDC’s statutory authority and violates the procedures required for agency rulemaking.”
The Biden administration responded late Monday with a statement saying that the agencies are reviewing the decision and assessing possible next steps. * * *
The CDC recommended that people continue to wear masks in indoor public transportation settings.
United, American, Southwest, Delta and Alaska and other airlines late Monday said they were dropping their face mask requirement effective immediately given a federal judge’s ruling in Florida and the White House response to it.
From the Medicare front, the Centers for Medicare Services announced
a proposed rule for inpatient and long-term hospitals that builds on the Biden-Harris Administration’s key priorities to advance health equity and improve maternal health outcomes. In addition to annual policies that promote Medicare payment accuracy and hospital stability, the FY 2023 Inpatient Prospective Payment System (IPPS) and Long-Term Care Hospital (LTCH) Prospective Payment System (PPS) rule includes measures that will encourage hospitals to build health equity into their core functions, thereby improving care for people and communities who are disadvantaged and/or underserved by the healthcare system. The rule includes three health equity-focused measures in hospital quality programs, seeks stakeholder input related to documenting social determinants of health in inpatient claims data, and proposes a “Birthing-Friendly” hospital designation.
For acute care hospitals paid under the IPPS that successfully participate in the Hospital Inpatient Quality Reporting Program and are meaningful electronic health record users, the proposed increase in operating payment rates is projected to be 3.2%. This reflects a FY 2023 projected hospital market basket update of 3.1% reduced by a projected 0.4 percentage point productivity adjustment and increased by a 0.5 percentage point adjustment required by statute. Under the LTCH PPS, CMS expects payments to increase by approximately 0.8% or $25 million. * * *
The American Hospital Association’s statement on the proposed rule may be found here. The regulatory battle has been joined.
From the medical research front
Medpage Today offers access to “a video [in which], Scott Weiner, MD, MPH, director of the Brigham Comprehensive Opioid Response and Education (B-CORE) Program at Brigham and Women’s Hospital in Boston, discusses his recent study on the risks of chronic use and overdose with hydrocodone versus oxycodone and how providers can keep their patients safe when prescribing these medications.” A transcript of the video also is provided.
Higher levels of “good” cholesterol in the fluid surrounding your brain and spinal cord may help protect you from Alzheimer’s disease, a new study suggests.
“This study represents the first time that small HDL particles in the brain have been counted,” said study co-author Dr. Hussein Yassine. He is an associate professor of medicine and neurology at the University of Southern California’s Keck School of Medicine in Los Angeles.
For the study, Yassine and his colleagues analyzed concentrations of high-density lipoproteins (HDL) — often referred to as “good cholesterol” — in the cerebrospinal fluid of 180 healthy volunteers with an average age of nearly 77.
The study linked a higher number of small HDL particles in cerebrospinal fluid with two key indicators that they might protect against Alzheimer’s. * * *
The results suggest that small HDL particles may point the way to treatments for early Alzheimer’s, long before mental decline occurs.
The nation’s preeminent cancer hospitals are charging commercial health insurers anywhere from double to seven times their costs of acquiring cancer drugs, a new study shows.
Most top cancer institutions also are keeping their drug prices secret in direct violation of federal law, potentially exposing themselves to fines.
The findings reinforce how cancer care, especially the drugs, generates significant revenue for hospitals, and how markups on drugs potentially put insured cancer patients in financially perilous situations. * * *
Ultimately, researchers found the amount of money that a hospital gets from an insurance company, just for the cancer therapy, often is more than what the drug company receives.
From the Capitol Hill front, today, the Senate took the following action
PN1166: Krista Anne Boyd, of Florida, to be Inspector General, Office of Personnel Management– Considered by Senate.– Confirmed by the Senate by Voice Vote.
And just like that, OPM has a Senate-confirmed Inspector General for the first time in over six years. The FEHBlog wishes Inspector General Boyd good luck.
The President issued a statement on World Health Day, which was celebrated today.
From the Omicron and siblings front —
The Centers for Medicare Services released an updated Toolkit on Covid Vaccines for health insurers and Medicare Advantage plans.
A federal appeals court has reinstated President Biden’s COVID-19 vaccine mandate for the federal workforce, overturning a lower court’s nationwide pause that had been in effect since January.
The plaintiffs who brought their suit over Biden’s executive order did not have standing in the federal circuit, a panel of the U.S Court of Appeals for the Fifth Circuit said in a 2-1 opinion Thursday evening, and instead must pursue their appeals through the Merit Systems Protection Board or Office of Special Counsel as laid out in the Civil Service Reform Act. The court vacated the injunction and instructed the district court in Texas that issued it to dismiss the case upon remand.
Medicare on Thursday finalized its plan to restrict coverage for the controversial, pricey Alzheimer’s drug Aduhelm to patients participating in clinical trials.
The decision marks the end of an intense pressure campaign from drugmakers and some patient groups who wanted Medicare to reverse its initial proposal and pay for the drug for more patients. As clinical trials are usually run out of major medical centers, the decision will likely mean some interested patients won’t be able to access the drug. However, Medicare isn’t explicitly requiring that patients be treated at hospital-based clinics like the initial proposal.
The decision has implications beyond Aduhelm’s manufacturer, Biogen, as well. The coverage decision is not specific to Aduhelm, and applies to all drugs in the class, including a forthcoming treatment that Eli Lilly has begun to submit for FDA approval.
But in a major change from the initial proposal, Medicare officials created a sort of shortcut path for drugs that, unlike Aduhelm, demonstrate a clinical benefit for patients before they are approved. Medicare will cover those medicines for a broader group of patients.
They would still need to collect some data, but the possible design of the studies is much more flexible — a significant win for Lilly.
Here is a link to the CMS fact sheet on this decision.
U.S. News adds “Medicare said Thursday it’s considering a cut in enrollee premiums after officials stuck with an earlier decision to sharply limit coverage for a pricey new Alzheimer’s drug projected to drive up program costs.” Given Medicare’s shaky financial condition, one would expect the government to build up reserves with the additional cash and then adjust the premium for the following Medicare year, taking all considerations into account.
From the No Surprises Act front, AHIP released a new resource reflecting on the first 100 days of the NSA.
From the healthcare business front, Fierce Healthcare informs us
[Blue Cross of California and Walgreen] are launching new Health Corners in 12 Walgreens stores in the San Francisco Bay area and Los Angeles County.
At the Health Corner locations, Blue Shield members and customers will be able to connect with health advisers who can offer simple in-store care as well as assistance with preventive screenings, chronic care management and medications. The health advisers have clinical backgrounds, such as pharmacists or nurse practitioners.
The partnership seemed a natural fit, D.D. Johnice, vice president of the Health Transformation Lab at Blue Shield of California, said in an interview. * * * Some 80% of people in California live within five miles of a Walgreens store, she said, so the Health Corners could be a valuable tool for reaching people who live in healthcare deserts, or more specifically, Blue Shield network deserts.”
Michael F. Neidorff, who as chief executive officer of Centene Corp. transformed a tiny medical insurance firm serving three counties in 1996 into a nationwide giant in government-backed health coverage, died Thursday after what his family described as a long illness. He was 79.
Mr. Neidorff recently took medical leave and had signaled last year a plan to retire in 2022 from the CEO job he held for more than 25 years. Centene announced in March the appointment of Sarah London, who had been vice chairman, to succeed him as CEO.
St. Louis-based Centene is the biggest company in managed Medicaid, contracting with states to provide coverage to people enrolled in the program for lower-income Americans.
Centene offers FEHB HMO coverage through its Health Net subsidiary. RIP.
Senate negotiators have reached agreement on a $10 billion pandemic relief package that includes funding for domestic needs but not international aid, according to two Senate aides who were not authorized to speak publicly.
The deal crystallizes an informal “agreement in principle” the parties reached last week to provide $10 billion for near-term pandemic needs by repurposing unspent funds from prior relief laws.
The White House backed the deal and urged Congress to pass the bill promptly, while noting it was less than the $22.5 billion the administration had requested for vaccines, boosters, treatments and testing.
“We will continue to work with Congress to fund our remaining domestic needs,” said Press Secretary Jen Psaki in a statement. She added that the White House would continue to press for funding global vaccination efforts.
The FEHBlog noticed that the Senate Homeland Security and Governmental Affairs Committee held a business meeting last Wednesday. The Committee favorably reported the President’s nomination of Kristin Boyd to be OPM Inspector General by voice vote (with Sen. Hawley (R Mo.) voting no). The next step for Ms. Boyd’s nomination is the Senate floor.
Last week, the House of Representatives passed a Secure 2.0 bill applicable to private sector defined contribution plans. The Senate is likely to approve the bill too. The Society for Human Resource Management has reviewed the bill’s provisions.
From the Omicron and siblings front —
Becker’s Hospital Review informs us “The World Health Organization is monitoring a new omicron variant — dubbed XE — that’s a hybrid of BA.1, the original omicron strain, and BA.2, a highly transmissible subvariant.” The hybrid is estimated to be 10% more contagious that BA.2.
American Hospital Association tells us “Beginning today through the end of the public health emergency, Medicare Part B beneficiaries may obtain up to eight free over-the-counter COVID-19 tests per month through eligible health care providers and pharmacies, the Centers for Medicare & Medicaid Services announced.” Medicare Part B beneficiaries can obtain the free tests by showing their Medicare identification card.
The American Medical Association discusses “How we will know when COVID-19 has become endemic.” The FEHBlog tends to think that we are there.
The Centers for Disease Control announced
The new nationwide Test to Treat initiative provides quick access to free treatment for COVID-19. Through this program, people can get tested and – if they are positive and treatments are appropriate for them – receive a prescription from a health care provider, and have their prescription filled all at one location. These “One-Stop Test to Treat” sites are available at hundreds of locations nationwide, including pharmacy-based clinics, federally qualified health centers, and long-term care facilities. People can continue to be tested and treated by their own health care providers who can appropriately prescribe these oral antivirals at locations where the medicines are distributed. A call center 1-800-232-0233 is available every day from 8:00 am to midnight ET to get help in more than 150 other languages. The Disability Information and Access Line is available to help people with disabilities access services. Call 1-888-677-1199, Monday-Friday from 9:00 am to 8:00 pm ET or email DIAL@usaginganddisability.org.
From the CMS front, the agency announced that “the updated MMSEA Section 111 GHP User Guide version 6.5 has been posted to the GHP User Guide page on CMS.gov. Refer to Chapter 1 for a summary of updates.” Section 111 is a system that has been in place for about 12 years. Section 111 helps CMS keep tabs on Medicare beneficiaries and beneficiaries using data group health plans, including FEHB plans, automobile and liability insurers, and attorneys for injured Medicare beneficiaries.
CMS also released “the Announcement of Calendar Year (CY) 2023 Medicare Advantage (MA) Capitation Rates and Part C and Part D Payment Policies (the Rate Announcement).”
From the federal employment front, Govexec reports
Federal employees can hold elected partisan office while also working at their agencies, a key panel found in a ruling setting a new precedent for civil servants.
Rodney Cowan did not have to give up his role as a county commissioner in Tennessee or be removed from his job with the U.S. Postal Service, the recently reconstituted central body of the Merit Systems Protection Board said in a decision last week. It was one of the first decisions of MSPB’s central board as it addresses its backlog of more than 3,500 cases that have piled up during its five years without a quorum.
The FEHBlog doubts that we have heard the last word on this issue.
The House of Representatives will engage in limited Committee business this week while the Senate will convene for Committee business and floor voting. Indeed, tomorrow the Senate will resumes consideration of the motion to proceed to H.R.3076, Postal Service Reform Act of 2022.
The Wall Street Journal observes that Congress has passed several bills on a bipartisan basis since the President’s Build Back Better plan stalled on Capitol Hill.
Already, bills to make the U.S. Postal Service more financially viable, boost U.S. competitiveness with China and ban mandatory arbitration in cases of sexual assault and harassment have picked up steam in Congress. Senators passed the arbitration bill by voice vote, sending it to the president’s desk without a single member of either party demanding a roll call to record yeas and nays.
Legislators also announced an agreement on a framework for legislation to fund the federal government through fiscal year 2022, and a deal to reauthorize a landmark domestic-violence bill, which lapsed in 2019.
Pretty, pretty good.
From the national health emergency front, Vox tells us the latest about the second Omicron variant, and The New York Times’ Morning column reviewed the disgraceful course of our country’s opioid epidemic. The article concludes
“The solutions are costly. A plan that President Biden released on the campaign trail, which experts praised, would total $125 billion over ten years. That’s far more than Congress has committed to the crisis. Lawmakers haven’t taken up Biden’s plan, and the White House hasn’t pushed for it, so far embracing smaller steps.
“But inaction carries a price, too. Overdose deaths cost the economy $1 trillion a year in health expenses, reduced productivity and other losses, a new report concluded — equivalent to nearly half of America’s economic growth last year.”
While the FEHBlog has not read the President’s plan, he does believe that a solution is desperately needed.
From the healthcare business front, Fierce Healthcare reviews the fourth quarter of 2021 financial results of significant health payers. At the top of the head were United Health Group and CVS Health /Aetna. “Both healthcare giants expect to top $300 billion in revenue this year, according to their forecasts.”
From the compliance front, Healthcare Dive reports
An analysis of 1,000 U.S. hospitals found that only 14.3% were complying with federal price transparency rulesand about 38% of hospitals posted a “sufficient amount of negotiated rates” on their websites.
The PatientRightsAdvocate.org analysis follows a report in July 2021 that showed only 5.6% of 500 random hospitals were in compliance with the rules that were introduced at the start of 2021.
“The largest hospital systems are effectively ignoring the law with no consequences,” the 61-page report said, noting that only two hospitals of 361 at three of the largest hospital systems were in compliance.
The FEHBlog wonders whether compliance would be higher if the compliance deadline (January 1, 2021) had not been at the height of a COVID surge in the ongoing pandemic.
From the preventive care front, the FEHBlog noticed in Health Payer Intelligence a Medicare national coverage determination on lung cancer screening that aligned Medicare coverage with a 2021 U.S. Preventive Services Task Force B graded recommendation.
This in turn reminded the FEHBlog that FEHB plans must cover all 21 USPSTF A and B graded recommendations made in 2021 with no member cost-sharing when delivered in-network beginning January 1, 2023. The FEHBlog counted a dozen such 2021 recommendations in the USPSTF list. Standing alone, those are a lot of changes to include in the 2023 benefit and rate proposals at the end of May 2022.
From the general healthcare front, NPR explains that the surprising details of the 65-year-old actor and comedian Bob Saget disclosed last week illustrate the importance of seeking immediate medical attention if you suffer a blow to your head.
According to his family, [Mr. Saget] “accidentally hit the back of his head on something, thought nothing of it and went to sleep.” No drugs or alcohol were involved, according to a coroner’s report.
Saget had “fractures to the back of his head and around his eyes” at the time of his death, according to an autopsy report from the Orange County, Fla., medical examiner obtained by People. Saget was also COVID-19 positive at the time of his death, the autopsy noted.
While details of how exactly Saget hit his head were not released, doctors stress the importance of seeking medical care immediately if you sustain a head or brain injury.
If you are concerned that you may have a head injury, consider getting yourself checked out,” said Dr. Amit Sachdev, medical director in the department of neurology at Michigan State University.
“Unfortunately, it’s all too common and we in neurology see it quite frequently that head injuries lead to bleeding,” said Sachdev.
Based on the CDC’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s latest chart of weekly new Covid cases from the 27th week of 2021 through the 6th week of 2022.
The chart shows a steep drop in Covid cases this year. Yet, according to the CDC, the rate of Omicron transmission remains high across our country. The CDC also reports
The current 7-day daily average for February 2–February 8, 2022, was 12,099 [new Covid hospitalizations]. This is a 25.4% decrease from the prior 7-day average (16,212) from January 26–February 1, 2022.
For the reasons explained in this Medscape article, the weekly count of Covid deaths continues to increase.
Finally, here is the FEHBlog’s chart of weekly Covid vaccinations distributed and administered.
New vaccinations, including boosters, have run under four million weekly for the past two weeks.
Here is a link to the CDC’s weekly review of its Covid statistics. The CDC’s critical observation is as follows:
COVID Data Tracker shows that as of February 10, 2022, about 213.4 million people, or 64.3% percent of the total U.S. population, have received a primary series of a COVID-19 vaccine.
However, only about half of those eligible to receive a booster dose have done so. Everyone ages 12 years and older should get a booster shot after they have completed their COVID-19 vaccine primary series. Omicron is extremely contagious, and even though overall severity is lower, the high volume of hospitalizations has strained the healthcare system. Being up to date with vaccination, in coordination with other key prevention strategies, is critical for preventing severe illness from COVID-19 and for reducing the likelihood of new variants from emerging. Find a vaccine provider and get your booster dose as soon as you can.
CDC’s Fluview adds “Sporadic influenza activity continues across the country.” The 2021 and 2002 winters have featured many Covid infections, but not that many flu infections.
U.S. drug regulators authorized the use of a new Covid-19 antibody drug from Eli Lilly & Co. that retains effectiveness against the Omicron variant of the virus, filling a void after authorities stopped distributing some older antibody drugs that lost effectiveness against the strain.
The Food and Drug Administration on Friday cleared the drug, bebtelovimab, for the treatment of mild to moderate Covid-19 in nonhospitalized individuals 12 and older who are at high risk of getting severely sick. The drug is intended for people who can’t get access to alternative Covid-19 treatments, or for whom those treatments aren’t appropriate.
Yesterday, the Biden administration announced the purchase of 600,000 courses of this drug.
From the Covid vaccine front, the Journal further reports that the Food and Drug delayed consideration of granting emergency use authorization to the Pfizer BioNTech Covid vaccine for children ages six months through four years.
The FDA had been considering a request by the companies to clear the use of two doses of the vaccine. The agency was then going to look at expanding the authorization to a third dose, should the study show it works safely.
Pfizer and BioNTech said they expect results on whether three doses of the vaccine works safely in early April. Researchers are collecting more data, including from more children in the study who have become infected as more time has passed.
The FEHBlog, who has young grandchildren, honestly does not understand why the government has been pushing so hard to vaccinate this age group.
From the opioid epidemic front, the American Medical Association informs us
The New York Times (2/10, Hoffman) reports that on Thursday, the CDC “proposed new guidelines for prescribing opioid[s]…that remove its previous recommended ceilings on doses for chronic pain patients and instead encourage doctors to use their best judgment.” Although they are “still in draft form, the 12 recommendations…are the first comprehensive revisions of the agency’s opioid prescribing guidelines since 2016,” and “they walk a fine line between embracing the need for doctors to prescribe opioids to alleviate some cases of severe pain while guarding against exposing patients to the well-documented perils of opioids.”
The AP (2/10, Stobbe) reports that the proposed changes are “contained in a 229-page draft update in the Federal Register,” and “the CDC will consider comments before finalizing the updated guidance.”
The Washington Post (2/10, Bernstein) reports that in a statement, AMA Board of Trustees Chair Bobby Mukkamala, M.D., said, “for nearly six years, the AMA has urged the CDC to reconsider its problematic guideline on opioid prescriptions that proved devastating for patients with pain. The CDC’s new draft guideline – if followed by policymakers, health insurance companies and pharmacy chains – provides a path to remove arbitrary prescribing thresholds, restore balance and support comprehensive, compassionate care.”
From the quality metrics front, NCQA released its proposed HEDIS and CAHPS changes for the 2023 measurement year today. NCQA is proposing to retire the CAHPS flu vaccination measure, which currently is included in OPM’s set of QCR measures used in the Plan Performance Assessment program. NCQA’s public comment period on the proposed changes closes on March 11.
In a move hailed by pharmacies, the U.S. Federal Trade Commission plans to vote later this month on whether to examine pharmacy benefits managers and how their controversial practices affect independent and specialty pharmacy operations.
The agency disclosed the planned Feb. 17 vote in a brief notice that specified interest in the “competitive impact of contractual provisions and reimbursement adjustments, and other practices affecting drug prices,” but did not provide any further detail. An FTC spokesperson wrote us that additional information will not be released until the upcoming meeting.
The FEHBlog will keep an eye on this vote.
From the Aduhelm front, Health Payer Intelligence discusses AHIP’s comments supporting CMS’s decision to provide very limited coverage of this drug in Medicare.
From the healthcare business front, Fierce Healthcare reports
Kaiser Permanente [the third largest carrier in the FEHB Program] reported $3 billion in net income for the second quarter of the year as membership in its health plan remains steady.
The health system and insurer posted total operating revenues of $23.7 billion against total operating expenses of $23.3 billion. The revenue was slightly above the $22.1 billion it earned in the second quarter of 2020.
Kaiser noted in its earnings statement Friday that favorable financial market conditions resulted in $3 billion in net income, compared with $4.5 billion for the second quarter of 2020.
“The COVID-19 health threat is not over, and we will continue to focus our resources on providing needed care for our patients and increasing vaccination rates to protect the health and safety of our workforce, members and the communities we serve,” said Kaiser CEO Greg Adams in a statement.
If you have time over the Super Bowl weekend, listen to or read Econtalk host Russ Robert’s discussion with macroeconomist John Taylor about inflation. Mr. Taylor created the Taylor Rule “that prescribes a value for the federal funds rate—the short-term interest rate targeted by the Federal Open Market Committee (FOMC)—based on the values of inflation and economic slack such as the output gap or unemployment gap.”
Happy Groundhog Day! The Pittsburgh Post Gazette informs us that “There will be six more weeks of winter, Punxsutawney Phil predicted as he emerged from his burrow Wednesday morning to perform his Groundhog Day duties.”
From the White House, we have the President’s fact sheet on his Cancer Moonshot initiative. Federal Times also has a report on today’s announcement.
A STAT News article on cancer markers suggests that the President’s timing may be right
Back in 2000, when President Clinton called a tie in the race to map the human genome, scientists forecasted a medicinal revolution, one in which scientists could ferret out the genetic roots of every known cancer and match patients with personalized treatments.
That did not happen, for reasons of biological complexity, technological immaturity, and perhaps a little scientific hubris. But after two decades of mapping the kaleidoscopic details of human DNA, researchers believe they finally have the tools and techniques to live up to those lofty promises.
“It’s almost like back to the future,” said Anna Barker, an oncologist who serves as chief strategy officer at the Ellison Institute for Transformative Medicine of USC. “Where we would like to have been 21 years ago is where we are now.” * * *
But many cancers don’t fit neatly into the field’s existing paradigm, said Suzanne Topalian, professor of surgery and oncology at Johns Hopkins University School of Medicine. Improving outcomes for those tumors will rely on multidimensional biomarkers, measurements that can take a systematic look at how cancer evolves rather than providing a snapshot.
To Barker, the field’s next major challenge is to find better biomarkers for “the big killers,” diseases including pancreatic cancer and glioblastoma.
“These are the cancers that — what are the unknown unknowns here? What are we missing?” she said. “We can’t seem to detect them early enough to stop them.”
From the opioid epidemic front, the National Institutes of Health informs us that
A new study of intentional drug overdose deaths, or suicides by an overdose of a medication or drug, found an overall decline in recent years in the United States, but an increase in young people aged 15-24, older people aged 75-84, and non-Hispanic Black women. The study also found that women were consistently more likely than men to die from intentional drug overdoses, with the highest rates observed in women ages 45 to 64. In addition, factors such as time of year, length of day, and day of the week appeared to be associated with intentional overdose death rates. The study published today in the American Journal of Psychiatry and was led by investigators at the National Institute on Drug Abuse (NIDA), part of the National Institutes of Health.
Nearly 92,000 people died from drug overdoses overall in the U.S. in 2020. This represents the largest increase ever recorded in a calendar year and reflects a nearly five-fold increase in the rate of overdose deaths since 1999. About 5% to 7% of these overdose deaths are recorded as intentional. Because it can be difficult to determine whether overdose deaths are intentional, the actual numbers are likely even higher. Many people who have a substance use disorder also develop other mental illnesses, such as mood and anxiety disorders, which are independently associated with increased suicide risk. In addition, many people who are diagnosed with other mental illnesses are often diagnosed with a substance use disorder, emphasizing the need to address co-occurring mental health conditions holistically.
“The distinction between accidental and intentional overdose has important clinical implications, as we must implement strategies for preventing both,” said Nora Volkow, M.D., senior author on the study and director of NIDA. “To do so requires that we screen for suicidality among individuals who use opioids or other drugs, and that we provide treatment and support for those who need it, both for mental illnesses and for substance use disorders.”
From the antibiotic resistance (“AR”) front, we learn that the CDC has updated its AR investment map.
“Highlights of this year’s AR Investment Map release include:
An interactive map showcasing CDC’s antibiotic resistance funding to support activities in every U.S. health department and across hundreds of public health partners
An updated fact sheet featuring CDC’s global investments with partners in more than 50 countries to improve detection, prevention, and response to AR threats internationally
An updated fact sheet showing how CDC’s COVID-19 efforts have also worked to address antibiotic resistance, including investments in infection prevention and control, training, surveillance, and public health personnel.”
Obviously, this is an important government initiative.
Anthem is betting on a different strategy than some of its competitors as it looks to transition to value-based care.
The payer is partnering with many value-based clinical platforms like Privia and CareMax to bring physicians into alternative payment models aiming to reimburse for the quality of care delivered, as opposed to pure volume. That’s a different tack on value-based primary care than its peers like UnitedHealth and Humana, which have mostly acquired and built their own clinical networks.
But Anthem is betting its capital-light strategy is more sustainable and flexible as the payer looks to push deeper into capitation to really bend the cost curve.
Walmart has partnered with a healthcare machine intelligence company to offer a personalized provider recommendation tool to associates who receive healthcare coverage through the retail giant’s health plan.
The company, Health at Scale, will provide the technology that Walmart intends to integrate into its health plan administrator’s search engine and virtual care referrals, according to the press release.
Associates and their families who are enrolled in Walmart’s health plan and work at select locations will have access to the resource, which aims to facilitate the process of finding a healthcare provider that fits a member’s health needs.
From the Rx coverage front, the always thought provoking Drug Channels opines that
The boffins at the Centers for Medicare & Medicaid Services (CMS) recently dropped the latest National Health Expenditure (NHE) data, which measures all U.S. spending on healthcare. (See links below.) These data provide our first official look at how the pandemic has affected U.S. healthcare spending.
Today, I examine the key insights from these latest figures.
As you will see, outpatient drug spending remains a small—and shrinking—share of the $4.1 trillion spent on U.S. healthcare. What’s more, drug spending again grew more slowly than overall healthcare spending.
Meanwhile, consumers shoulder a much higher portion of this spending compared with their share of hospital spending.
Speaking of CMS that agency today released “the Calendar Year (CY) 2023 Advance Notice of Methodological Changes for Medicare Advantage (MA) Capitation Rates and Part C and Part D Payment Policies (the Advance Notice). CMS will accept comments on the CY 2023 Advance Notice through Friday, March 4, 2022, before publishing the final Rate Announcement by April 4, 2022.” Here’s a link to the CMS fact sheet.
The FEHBlog wishes that OPM would release a draft call letter for carrier comment before finalizing it. In fairness OPM does solicit carrier input before it draft the call letter. Nevertheless, it would be more collaborative for OPM to seek carrier comment before drafting and then on the first draft.
From the HR front, Federal News Network reports that
A new memo from the Office of Personnel Management released today, offers them performance management tips for a hybrid workplace.
“Effective performance management requires engagement and commitment from individuals at all levels of an agency,” the memo says. “As such, these performance management tips have been uniquely tailored to assist Non-supervisory Employees, Supervisors, and Leadership throughout the various phases of the performance management cycle.”
And now with agencies expected to begin returning employees to the office in the coming months, OPM wants to make sure managers are “equipped to manage employee performance equitably and effectively—regardless of whether the employees are in the office or not.”
From the Omicron front, Live Science informs us about the so-called stealth Omicron variant.
A stealthy version of the omicron variant has been detected in the U.S., but so far, it makes up a very low proportion of the overall cases in the country.
This version of the variant, called BA.2, bears some genetic mutations not seen in the original omicron lineage, and some of these mutations lie in the spike protein, according to the World Health Organization (WHO). Some preliminary data hint that BA.2 may be slightly more transmissible, but not more severe, than the original omicron, but it’s too early to interpret that data with any confidence.
In December, scientists reported that the original version of omicron had split into multiple sublineages, one of these being BA.2, Live Science previously reported. BA.2 bears a genetic quirk that makes it harder to track using PCR tests, so it’s been nicknamed “stealth omicron.”
The New York Times tells us about a new study identifying four factors that may lead to “Long Covid“.
The researchers said they had found that there was an association between these factors and long Covid (which goes by the medical name post-acute sequelae of Covid-19, or PASC) whether the initial infection was serious or mild. They said that the findings might suggest ways to prevent or treat some cases of long Covid, including the possibility of giving people antiviral medications soon after an infection has been diagnosed. * * *
One of the four factors researchers identified is the level of coronavirus RNA in the blood early in the infection, an indicator of viral load. Another is the presence of certain autoantibodies — antibodies that mistakenly attack tissues in the body as they do in conditions like lupus and rheumatoid arthritis. A third factor is the reactivation of Epstein-Barr virus, a virus that infects most people, often when they are young, and then usually becomes dormant.
The final factor is having Type 2 diabetes, although the researchers and other experts said that in studies involving larger numbers of patients, it might turn out that diabetes is only one of several medical conditions that increase the risk of long Covid.
The COVID-19 booster drive in the U.S. is losing steam, worrying health experts who have pleaded with Americans to get an extra shot to shore up their protection against the highly contagious omicron variant.
Just 40% of fully vaccinated Americans have received a booster dose, according to the Centers for Disease Control and Prevention. And the average number of booster shots dispensed per day in the U.S. has plummeted from a peak of 1 million in early December to about 490,000 as of last week.
Also, a new poll from The Associated Press-NORC Center for Public Affairs Research found that Americans are more likely to see the initial vaccinations — rather than a booster — as essential.
“It’s clear that the booster effort is falling short,” said Jason Schwartz, a vaccine policy expert at Yale University. * * *
As for why an estimated 86 million Americans who have been fully vaccinated and are eligible for a booster have not yet gotten one, Schwartz said public confusion is one important reason.
“I think the evidence is now overwhelming that the booster is not simply an optional supplement, but it is a foundational part of protection,” he said. “But clearly that message has been lost.”
The need for all Americans to get boosters initially was debated by scientists, and at first the government recommended only that certain groups of people, such as senior citizens, get additional doses. The arrival of omicron, and additional evidence about falling immunity, showed more clearly a widespread need for boosters.
But the message “has been lost in the sea of changing recommendations and guidance,” Schwartz said.
Speaking of confusion over boosters, Kaiser Health News reports that
The Centers for Disease Control and Prevention reached out to pharmacists Wednesday to reinforce the message that people with moderate to severe immune suppression are eligible for fourth covid shots.
The conference call came a day after KHN reported that immunocompromised people were being turned away by pharmacy employees unfamiliar with the latest CDC guidelines.
If you thought that the idea of mixing and matching Covid boosters was confusing, the National Institutes of Health reassureed us that
In adults who had previously received a full regimen of any of three COVID-19 vaccines granted Emergency Use Authorization (EUA) or approved by the U.S. Food and Drug Administration, an additional booster dose of any of these vaccines was safe and prompted an immune response, according to preliminary clinical trial results reported in The New England Journal of Medicine. The findings served as the basis for recommendations by the FDA and the Centers for Disease Control and Prevention in late fall 2021 to permit mix-and-match COVID-19 booster vaccinations in the United States. Additional data from the ongoing Phase 1/2 trial, sponsored by the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health, are expected in the coming months.
From the Postal Service front, Govexec reports that
USPS, like the rest of the nation, has experienced a surge in COVID-19 cases from the omicron variant and thousands of workers are sick or quarantining each day. Still, the agency oversaw a largely successful holiday period and continues to ramp up its delivery of COVID-19 rapid tests on behalf of the administration. The Health and Human Services Department is reimbursing USPS for its costs, but the Postal Service has declined to disclose the terms of that arrangement. The mailing agency has kept on thousands of temporary staff to support the effort and is using its own facilities to stage the shipments. Tens of millions of tests have already gone out, White House Coronavirus Response Coordinator Jeff Zients said on Wednesday.
Zients added the administration opted against using USPS to distribute 400 million N95 masks from the National Stockpile because its alternative approach—sending them to pharmacies and other locations to give to customers for free—is quicker. The masks have already reached many facilities and Americans are picking them up.
From the hearing aid front, Roll Call reports on the state of the Food and Drug Administration’s efforts to craft a rule allowing hearing aids to be sold over the counter, a Biden Administration initiative. Suffice it to say that nothing is simple.
From the healthcare business front, Healthcare Dive tells us that
The fourth quarter results for Indianapolis-based Anthem were mixed, analysts said. The financial results released premarket Wednesday beat Wall Street expectations on earnings, but missed on operating revenue.
Higher-than-expected coronavirus-related costs driven by the omicron variant — most notably in December — were “more than offset” by lower utilization of non-COVID-19 care, CFO John Gallina told investors on a Wednesday morning call.
Anthem’s commercial business had the highest costs relative to baseline, driven by factors like children becoming eligible for COVID-19 vaccines and the omicron surge. Medicare was next in line, followed by Medicaid, which actually ended the quarter slightly below baseline, Gallina said. The CFO noted he expects that theme to continue in 2022.
The payer’s medical loss ratio, the percentage of premiums invested back into patient care, was 89.5% in the quarter, in line with analyst forecasts and up sequentially from the third quarter’s 87.7%, which was much lower than analysts had expected. The fourth quarter of the year typically has a higher MLR, even notwithstanding pandemic pressures.
The number of accountable care organizations participating in the Medicare Shared Savings Program (MSSP) modestly increased to 483 this year compared with 477 for 2021, sparking new worries from advocates over the future of the program.
The Centers for Medicare & Medicaid Services released new figures Wednesday that show the patient population being served by ACOs has slightly grown. The new data come as the Biden administration released a strategic refresh last year for its payment models with the intent of getting every Medicare beneficiary in an accountable care relationship by 2030. * * *
ACO advocates have been concerned about a decline in overall participation that has been occurring in the MSSP in recent years. There were 517 ACOs participating in 2020, which was up from the 519 that operated in 2019. However, that’s down significantly from the 561 that participated in 2018.
The National Association of ACOs (NAACOS) has previously called for CMS to make it easier for organizations to take on financial risk. The group criticized a Trump-era program called “Pathways to Success” that requires ACOs to take on financial risk much earlier in the process.
NAACOS has also called for greater predictability in ACO benchmarks that set the spending and quality targets ACOs must meet to qualify for shared savings as well as increases in such shared savings rates.
From the mental health parity front, Health Payer Intelligence digs into yesterday’s government report on health plan compliance with the federal mental health parity law.
Out of all of the comparative analyses that EBSA received, not a single payer provided all of the information that the review requested in the initial submission.
As a result, the administration sent out 80 letters to payers requesting more information. Twelve of the letters went to payers that had already received a letter from EBSA notifying them that they had submitted insufficient information and seeking the requested details.
EBSA still has not announced any final determinations. However, after this back and forth with payers, EBSA accrued enough information to find 30 health plans in non-compliance on a total of 46 NQTLs.
Three major issues stood out to EBSA as the administration assessed NQTL compliance.
First, the administration found that many health plans and issuers were not prepared for compliance. * * *
Second, the initial comparative analyses perpetuated a historic trend of providing insufficient data due to five types of errors. * * * [For example] payers did not perform a comparative analysis before designing their NQTLs, so the NQTLs were unlikely to meet EBSA’s standards. * * *
Finally, despite lack of preparation and a range of errors that led to a fragmentary picture of the NQTLs and their applications, EBSA found that some plans could receive an initial determination even for an incomplete analysis. Hence, 30 plans have already received initial determinations of non-compliance.
As EBSA continues the determinations, the administration recommended changes to Congress that would enhance enforcement of the mental health parity compliance law, promote access to coverage, and standardize compliance regulations.
The FEHBlog recommends reading the entire article. As the FEHBlog mentioned yesterday, the mental health parity law could be made simpler and more effective but that outcome is just not in the cards at least currently.
From the COVID vaccination front, the CDC’s COVID Data Tracker indicates that over two-thirds of the U.S. population over five years old in fully vaccinated.
The American Medical Association’s column about “What Doctors Wish Patient Knew” explains
A Kaiser Family Foundation poll found that one-third of parents say they planned to get their children vaccinated right away. Yet other parents are taking a wait-and-see approach to COVID-19 vaccination for kids. But with the Delta-Omicron variant tag team, widespread vaccination is an essential tool for preventing COVID-19 deaths, hospitalizations and illnesses.
To help parents move from that “wait-and-see” mentality and calm their fears, two physicians shared what to know about COVID-19 vaccine safety for children.
Check it out.
From the Omicron treatment front, the Food and Drug Administration announced today that the agency has
revised the authorizations for two monoclonal antibody treatments – bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab) [which are made by Eli Lilly & Co. and Regeneron Pharmaceuticals Inc.] – to limit their use to only when the patient is likely to have been infected with or exposed to a variant that is susceptible to these treatments.
Because data show these treatments are highly unlikely to be active against the omicron variant, which is circulating at a very high frequency throughout the United States, these treatments are not authorized for use in any U.S. states, territories, and jurisdictions at this time. In the future, if patients in certain geographic regions are likely to be infected or exposed to a variant that is susceptible to these treatments, then use of these treatments may be authorized in these regions.
Monoclonal antibodies are laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens such as viruses, like SARS-CoV-2. And like other infectious organisms, SARS-CoV-2 can mutate over time, resulting in certain treatments not working against certain variants such as omicron. This is the case with these two treatments for which we’re making changes today. * * *
Importantly, there are several other therapies – Paxlovid, sotrovimab, Veklury (remdesivir), and molnupiravir – that are expected to work against the omicron variant, and that are authorized or approved to treat patients with mild-to-moderate COVID-19 who are at high risk for progression to severe disease, including hospitalization or death. Healthcare providers should consult the NIH panel’s COVID-19 treatment guidelines and assess whether these treatments are right for their patients.
From the COVID vaccination mandate front, Federal News Network reports that
Last week’s court injunction that blocked the Biden Administration’s vaccine requirement for federal employees will put a temporary halt to disciplinary actions in federal agencies. But it won’t be of much help to feds who’d already been disciplined or fired for refusing the vaccine prior to last Friday.
That’s according to new guidance the administration’s Safer Federal Workforce Task Force issued Monday. The four-page document answers some basic questions on exactly how agencies should deal with the federal employee mandate now that a Texas judge has temporarily barred its implementation and enforcement.
Among the nuances: workers who’ve been suspended for failing to comply need to have their suspensions lifted, and new proposals to fire or suspend employees need to be “held in abeyance” for as long as the injunction is in place, the task force said. But agencies don’t need to reverse other disciplinary procedures that have already taken full effect.
From the free OTC tests front, Govexec.com asks
What group is especially vulnerable to the ravages of COVID-19 even if fully vaccinated and boosted? Seniors. And who will have an especially tough time getting free at-home COVID tests under the Biden administration’s plan? Yes, seniors.
As of Jan. 15, private insurers will cover the cost of eight at-home rapid COVID tests each month for their members — for as long as the public health emergency lasts.
Finding the tests will be hard enough, but Medicare beneficiaries face an even bigger hurdle: The administration’s new rule doesn’t apply to them.
It turns out that the laws governing traditional Medicare don’t provide for coverage of self-administered diagnostic tests, which is precisely what the rapid antigen tests are and why they are an important tool for containing the pandemic. * * *
The Medicare program does cover rapid antigen or PCR testing done by a lab without charging beneficiaries, but there’s a hitch: It’s limited to one test per year unless someone has a doctor’s order.
Because the article describes orignal Medicare as exempt, one must assume that Medicare Advantage plans also are offering reimbursement for OTC COVID tests. The original Medicare exemption is a weak cup of tea because no commercial health plans covered OTC testing before the mandate.
From the No Suprises Act front, The American Hospital Association informs us that
The Centers for Medicare & Medicaid Services will host a conference call for health care providers Jan. 26 at 1 p.m. ET on the balance billing provisions of the No Surprises Act. To participate in the Special Open Door Forum, dial 888-455-1397 and reference passcode 5109694. Slides for the call are available here. P
Participants may email questions in advance to Provider_Enforcement@cms.hhs.gov, noting “Questions for 1/26 Open Door Forum” in the subject line. A replay will be available after the call through Jan. 28 by dialing 800-308-7855 and entering the passcode.
The CMS slides are helpful.
From the telehealth front, Fierce Healthcare tells us that
Integrating virtual care can save the healthcare system significant amounts of money, as well as avoid unnecessary visits to the emergency department or urgent care center, according to a new study from Cigna.
The study, conducted alongside its telehealth arm MDLive, found that patients who saw virtual providers also saw 19% fewer visits to the ER or urgent care. In addition, virtual urgent care visits reduced duplication of care by 16% compared to other virtual primary care providers or specialists.
Cigna notes that these reductions in unneeded visits are especially crucial as hospitals face down the current COVID-19 surge, caused by the highly infectious omicron variant.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.