West Virginia Democrat Joe Manchin III is yet again upending his party’s priority economic package, jettisoning climate measures and tax increases he previously favored and leaving only provisions focused on lowering health care costs.
Manchin communicated the decision to his negotiating partner, Senate Majority Leader Charles E. Schumer, on Thursday, according to two Democratic sources familiar with the situation.
The move came one day after Manchin expressed heightened anxiety about inflation, after the June consumer price index data released that morning showed inflation climbed 9.1 percent on an annualized basis over the previous year.
The House on Thursday passed, 329-101, its version of the fiscal 2023 National Defense Authorization Act, which would authorize $840.2 billion in national defense spending, after sifting through hundreds of amendments and hours of debate.
The sprawling Pentagon policy bill, which has been enacted into law every year for the past 61 years, would authorize funds for the Defense Department and national security programs within the Department of Energy. * * *
In the coming months, the Senate will take up its own version of the annual defense policy bill.
This must-pass bill typically includes significant federal procurement changes that can impact FEHB contracts.
From the Omicron and siblings front, MedPage Today offers an expert opinion on whether to get a second Covid booster or wait until the fall for potentially improved Covid shots?
For those still deciding, the CDC’s booster calculator provides guidance for anyone unsure about their eligibility. Generally speaking, for people age 60 and older, a first booster is recommended for those who received primary immunization more than 5 months previously, and a second booster is recommended for those who received their first booster more than 4 months ago.
James Grisolia, MD, a San Diego neurologist, described it as a physician’s dilemma. “While we were between surges, I would have given similar advice (to wait before getting the second booster) but as of several weeks ago, it was obvious we were going into another surge. I began encouraging older folks to get their second booster.”
From the FEHB front —
Fedweek discusses the differences in levels of FEHB coverage.
Benefits consultant Tammy Flanagan wraps up her three-part series on one federal employee’s journey into retirement with an article on FEHB issues.
From the telehealth front, Healthcare Dive offers an interview with Teladoc’s chief medical officer, Vidya Raman-Tangella.
From the mental healthcare front, here is a link to SAMHSA’s 988 nationwide suicide/mental healthcare crisis hotline which becomes available on Saturday, July 16.
From the reports department
CVS Health released its Health Care Insights 2022 report.
The Kaiser Family Foundation issued a report on the cost of delivering a baby in the U.S. “This analysis examines the health costs associated with pregnancy, childbirth, and post-partum care using a subset of claims from the IBM MarketScan Encounter Database from 2018 through 2020 for enrollees in large employer private health plans. It finds that health costs associated with pregnancy, childbirth, and post-partum care average a total of $18,865 and the average out-of-pocket payments total $2,854.”
From the U.S. healthcare business front, MedPage Today identifies the largest physician groups in our country.
From the Capitol Hill front, STAT News provides more information on the Senate Democrats’ drug pricing proposal
The text released Wednesday is similar to a sweeping package that passed the House last year — it would allow Medicare to negotiate prices with drugmakers, it would protect seniors from especially exorbitant drug costs, and it would discourage drugmakers from raising their prices dramatically.
There are some notable changes that will affect when patients see savings, how the drug development pipeline works, how certain patients will pay for insulin, and how the new prices would affect safety-net programs and Medicaid.
The Washington Examiner emphasizes The proposal * * * lacks language included in the lower chamber’s bill that would cap insulin prices for people with diabetes at $35 a month.”
Senate Democrats are taking a gamble and removing all of the provisions that would have lowered patients’ insulin prices out of the bill, to allow a separate, bipartisan effort led by Sens. Jeanne Shaheen (D-N.H.) and Susan Collins (R-Maine) to advance.
Now, the HHS secretary would still be allowed to negotiate insulin prices, but only within the parameters and limits of the regular process. Shaheen and Collins’ bill relies on drugmakers voluntarily lowering their prices in exchange for banning rebates for the products.
The brand drug lobby PhRMA blasted the out-of-pocket cost changes, claiming that “Democrats weakened protections for patient costs included in previous versions, while doubling down on sweeping government price-setting policies.”
Six months after regulators issued an emergency use authorization for Paxlovid, physicians say they still have significant questions about prescribing guidelines for the leading treatment for high-risk Covid patients.
STAT spoke with providers who said they and their colleagues aren’t on the same page about when to prescribe Paxlovid or the criteria that separates those who need it from those who do not. They also said it is unclear whether they can give a second course when patients test positive again after taking Paxlovid, a phenomenon known as a rebound. And nearly all the experts who spoke with STAT said that they are clamoring for more data on rebounds, which is complicating and sometimes changing their calculus about when to give the drug.
“There is a real dearth of evidence right now out there, and obviously there’s a lot of confusion,” said Jonathan Li, a physician at Brigham and Women’s Hospital and virology researcher at Harvard Medical School who is also a member of the Covid-19 Treatment Guidelines Panel. “And even amongst people who are immersed in the literature, and who are infectious disease experts, you’ll see actually a fairly wide range in opinions.” * * *
“Pretty much everybody meets the EUA criteria. They made it very, very, very broad,” said David Smith, a professor, physician, and virology researcher at the University of California, San Diego. In a single week in May, over 160,000 Paxlovid prescriptions were filled.
Physicians generally agree that certain high-risk patients — including people who are unvaccinated or those over 65 with multiple comorbidities — should always be prescribed the drug. But the broader eligibility makes it difficult for some physicians to decide who should or should not receive Paxlovid. A child is not likely to need it, but what about a healthy 50-year-old man? A 65-year-old woman? The experts STAT spoke with didn’t agree.
According to Lawrence Kleinman, MD, MPH, of the department of pediatrics at Rutgers Robert Wood Johnson Medical School in New Jersey, we need to take our time in defining long COVID, whether it’s with a checklist, an algorithm, or an entry for the medical dictionary.
“If we defined it a certain way and we missed something in that initial definition, then there will be silence on that until someone comes around and does a postmortem on our analysis,” Kleinman, who is also the lead researcher in the Rutgers pediatric hub of the NIH’s nationwide RECOVER study, told MedPage Today. “We want to avoid that to the extent that’s possible.”
He said more research and data collection are needed before the work of defining long COVID is possible in a clinically meaningful way. At the moment, he noted, there isn’t even clear criteria for where to start.
For example, should researchers focus on setting a specific number of days a person experiences fatigue after an acute COVID infection? If so, what should those ranges look like — fatigue after 30 days? As he pointed out, there are not enough data to develop the foundational elements needed for researchers to piece together a practical definition just yet.
Nothing is simple.
From the Medicare front, the American Hospital Association reports
The Centers for Medicare & Medicaid Services today released its calendar year 2023 proposed rule for the physician fee schedule. The rule proposes to cut the conversion factor to $33.08 in CY 2023, as compared to $34.61 in CY 2022, which reflects the following: the expiration of the 3% statutory payment increase; a 0.00% conversion factor update; and a budget-neutrality adjustment. In addition, CMS proposes to delay for one year (until Jan. 1, 2024) the implementation of its policy to define the substantive portion of a split (or shared) visit based on the amount of time spent by the billing practitioner. Under this policy, if a non-physician practitioner performed at least half of an E/M visit and billed for it, Medicare would only pay 85% of the PFS rate.
CMS proposes numerous policy changes to the Medicare Shared Savings Program. For example, it would modify the manner in which accountable care organizations’ benchmarks are calculated to help sustain long-term participation and reduce costs. It also would provide increased flexibility for certain smaller ACOs to share in savings. The rule also proposes updates to MSSP quality-measurement policies, including a new health equity adjustment that would award bonus points to ACOs serving higher proportions of underserved or dually-eligible beneficiaries.
For the Quality Payment Program, CMS proposes five new, optional Merit-based Incentive Payment System Value Pathways that would be available beginning in 2023. These MVPs align the reporting requirements of the four MIPS performance categories around specific clinical specialties, medical conditions or episodes of care. CMS also proposes refinements to the MIPS subgroup reporting process, an increase to the quality data completeness threshold, and changes to the requirements and scoring of the Promoting Interoperability category. The proposed rule also includes requests for input on policy ideas for advancing health equity and transitioning to digital quality measurement.
The FDA suddenly reversed course this week on its efforts to ban Juul e-cigarette sales, an embarrassing about-face that calls into question the reasoning behind the agency’s initial decision, experts said.
Tuesday evening, the Food and Drug Administration announced it was giving Juul’s application for its vaping products a second look because of “scientific issues … that warrant additional review.” The move came less than two weeks after the FDA made international headlines for ordering all of the vaping giant’s products off the market, prompting praise from lawmakers and advocates alike.
The FDA previously said that Juul “did not provide [sufficient] evidence and instead left us with significant questions,” which prevented the agency from granting its application. But now, it seems, the FDA is acknowledging there is additional information in Juul’s application that regulators didn’t adequately consider.
Fertility benefits and family-building programs have become table stakes for employers looking to support their workforce, but an increasing number of providers and employees are working to offer care during the next stage of reproductive health: menopause.
Nine out of 10 working women said menopause affects their work performance, according to a survey by AARP, which estimates that companies lose $150 billion a year in lost productivity as a result. Yet, 99% of women in the U.S. don’t have access to an employer-sponsored menopause care benefit.
“This is an area that nobody has really focused on, and there isn’t much out there available for employees,” says Maya Bodinger, vice president of business development at P.volve. “The menopause transition can be anywhere from four years to 12. This is not just a year or two like how we traditionally think about reproductive health.”
Cesarean deliveries have increased in the U.S. over the last few years, driven by a rise in patients who underwent first-time C-sections, according to a CDC report.
While the rate of primary C-sections fluctuated from 2016 to 2019, it increased from 2019 to 2021 among women in all age groups, reported Michelle Osterman, MHS, of the CDC’s National Center for Health Statistics.
The repeat cesarean rate, however, which captures patients who have multiple procedures, steadily decreased by around 1% each year from 2016 to 2021 (87.6% to 85.9%), Osterman noted. Repeat cesarean delivery rates decreased specifically for women ages 25 to 39, those who identified as white or Hispanic, and those with full- or late-term pregnancies.
The increase in overall C-sections likely would have been higher if not for the decrease in repeat procedures, she said.
“Because 7 to 9 out of 10 pregnant folks with a prior cesarean will have a repeat cesarean, we can anticipate an overall climb in the overall cesarean delivery rate for the years ahead,” Kjersti Aagaard, MD, PhD, an ob/gyn at Baylor College of Medicine and Texas Children’s Hospital in Houston, told MedPage Today.
Finally, the FEHBlog notes that benefits consultant Tammy Flanagan has released the second part of her three-part story on a typical federal employee’s experience with the federal government’s retirement process. The report appears in Govexec.
Senate Democrats have narrowly reached a deal on legislation to give Medicare the power to negotiate for lower drug prices.
The Senate released text Wednesday (PDF) on the deal that also repeals the controversial Part D rebate rule and installs a cap on monthly cost-sharing payments for Part D and Medicare Advantage plans.
The legislative text shows that starting in 2026, the Department of Health and Human Services will choose 10 drugs eligible for negotiation. The next year, the number of eligible drugs will increase to 15, and in 2029 and every year after by 20.
The sole-source drugs subject to negotiation will be chosen based in part on their total spending under Medicare Parts B and D. There is an exception for small biotech drugs from 2026 through 2028 such as vaccines and excludes certain orphan drugs as well.
Roll Call adds “Congress is fast approaching its scheduled August recess, followed by peak campaign season, so Democratic lawmakers only have a few more weeks in session to push their legislative priorities before they could lose control of either chamber in November.”
From the Omicron and siblings front, the American Hospital Association tells us
The Food and Drug Administration today authorized state-licensed pharmacists to prescribe Paxlovid (nirmatrelvir and ritonavir) to patients as a treatment for those at high risk of severe COVID-19. Because Paxlovid must be taken within five days of symptom onset, the change could spur expanded access and more-timely treatment of eligible patients. The change was made through an amended emergency use authorization.
This standing order approach should accelerate the continuing rollout of test to treat locations.
Governments, drugmakers and vaccination sites are discarding tens of millions of unused Covid-19 vaccine doses amid sagging demand, a sharp reversal from the early days of the mass-vaccination campaign, when doses were scarce. * * *
In the U.S., about 90.6 million Covid-19 doses have been wasted, or 11.9% of the more than 762 million Covid-19 vaccine doses delivered since the shots became available in late 2020, according to the Centers for Disease Control and Prevention.
The wastage rate has accelerated recently: Some 12 million of the discarded doses have been thrown out since late May.
The disposals come during a significant drop in demand for Covid-19 vaccines, even with young children recently becoming eligible. The seven-day moving average of doses administered daily in the U.S. was about 155,000 as of June 21, down from about 1.1 million on Jan. 1 and the peak of about 3.5 million daily in April 2021.
Partly driving the wastage, health experts said, is the way the Covid-19 vaccines are packaged in multiuse vials containing from five to 20 doses. Once opened, the vials generally must be used within about 12 hours of opening or the remaining doses discarded.
From the telehealth front
Healthcare Dive reports
COVID-19 made its way back into the top five telehealth diagnoses nationally on Fair Health’s monthly tracker in April for the first time since January, according to the report out Wednesday.
Every U.S. census region except the South saw COVID-19 return to the top five diagnoses list, and the uptick is in line with rising cases reported in April by the Centers for Disease Control and Prevention.
Telehealth use overall also rose nationally and in every region after two months of decline, the report found.
Teladoc is further building out its primary care offering, Primary360, with new services that enhance care coordination and grow in-home options.
Primary360 will now provide care coordination support and health plan in-network referrals alongside free same-day medication delivery from Capsule and in-home, on-demand phlebotomy services backed by Scarlet Health, according to an announcement Wednesday from Teladoc.
The new care coordination capabilities will allow Primary360’s care team to take a “holistic” view of the patient’s coverage and make streamlined referrals to Teladoc services they can access. The care team can also then ensure a patient is referred to an in-network provider when in-person services are necessary.
mHealth Intelligence reports “The burgeoning mental health epidemic in America is widespread across age groups, but the youth have faced a particularly challenging time amid the COVID-19 pandemic. As the youth mental health crisis reaches new heights, providers are increasingly turning to telehealth to help expand access to behavioral healthcare.”
In the same spirit, Health Data Management discusses best practices for hospitals interested in providing acute care at home services.
From the U.S healthcare front, Beckers Hospital Review calls our attention to the fact that “Money, formerly Money Magazine, and Leapfrog Group collaborated for their first shared ranking of “best hospitals” to help consumers make decisions about which healthcare institutions are best for their money. The inaugural list was released July 6 and can be found in full here.” Check it out.
From the fraud, waste and abuse front, Healthcare Dive reports
The federal government won or negotiated more than $5 billion in healthcare fraud judgments and settlements in its 2021 fiscal year, the largest amount ever in the history of the HHS and Department of Justice’s fraud and abuse enforcement program.
Due to those and other efforts from previous years, the government clawed back almost $1.9 billion, according to a new report from the departments.
Of that $1.9 billion, about $1.2 billion went to the Medicare trust funds, which are on increasingly precarious financial footing due to growing stress on the insurance program. In addition, roughly $99 million in federal Medicaid money was transferred back to the CMS.
Finally, Govexec brings us up to date on projections for 2023 annual raises for federal employees.
President Biden and House appropriators seem thus far to be in agreement that federal employees should receive an average 4.6% pay raise next year, but there are still several steps officials must take before it can be implemented at the end of the year. * * *
On Capitol Hill, there are still a few opportunities for federal employee groups and some lawmakers to try to increase the raise to the average 5.1% figure they have been advocating for.
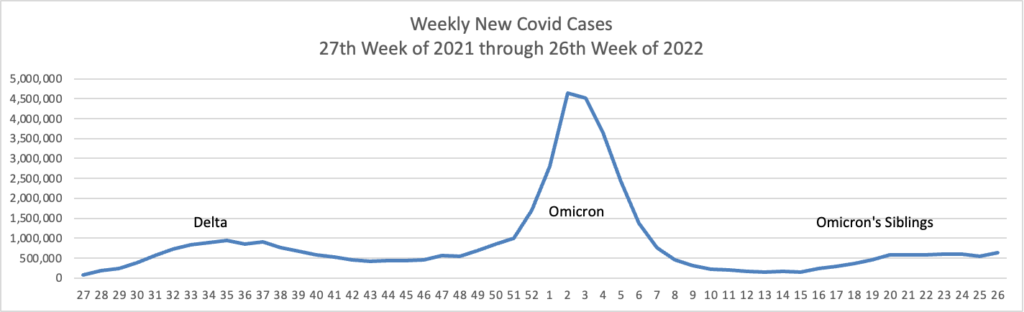
Using the CDC’s Covid Data Tracker and Thursday as the first day of the week, here are the FEHBlog’s weekly charts of new Covid cases and deaths from the 27th week of 2021 through the 26th week of 2022:
The CDC did not produce its weekly review of Covid statistics today as it’s the beginning of the July 4th holiday weekend. The CDC’s daily averages of new cases, new deaths and new hospitalization for the past week has been 109,944 cases, 316 deaths and 4,947 hospitalizations.
Temporary loss of smell emerged as a common indicator of COVID-19 early in the pandemic. Research into the cause and treatment of the condition, known as anosmia, is ongoing, though recent studies have brought us one step closer to answers.
Two latest findings on COVID-19-related anosmia:
1. Loss of smell and taste is becoming less common as the virus evolves, according to researchers.
2. Smell and taste hasn’t fully returned for many people who contracted COVID-19 early in the pandemic, research shows.
In retrospect, the FEHBlog is pleased that he continued theses charts from the last six months of 2021 into the first half of 2022 because doing so captured the three important surges. Now the FEHBlog has to decide what to do next Friday as the charts present a years worth of data.
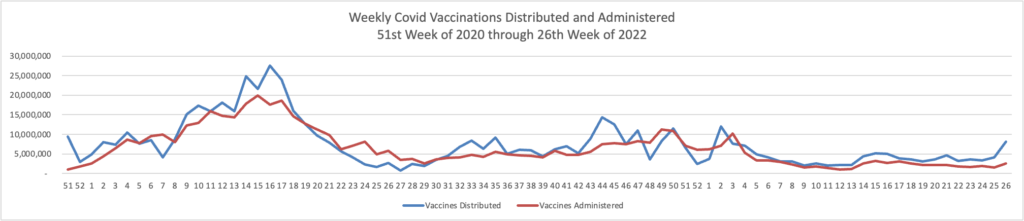
Here is the FEHBlog’s weekly chart of Covid vaccinations distributed and administered from the beginning of the Covid vaccination era (the 51st week of 2020) through this week, the 26th week of 2022.
It’s worth adding that the CDC is currenly providing weekly, not daily, vaccination stats. The CDC is now offering on a colorful, adjustable chart on “Primary Series Completion, Booster Dose Eligibility, and Booster Dose Receipt by Age, United States.
COVID-19 vaccines protected against severe disease and death in people with overweight or obesity, a large English study found.
Compared with the unvaccinated, vaccinated individuals in each BMI group experienced significantly lower likelihood of COVID-related hospitalization starting at 2 weeks from their second dose, reported Carmen Piernas, PhD, of the University of Oxford, and colleagues:
A new study provides more evidence that influenza vaccination may help protect older adults against Alzheimer’s disease (AD).
In a large propensity-matched cohort of older adults, those who had received at least one influenza inoculation were 40% less likely than unvaccinated peers to develop AD over the course of 4 years.
“Influenza infection can cause serious health complications, particularly in adults 65 and older. Our study’s findings ― that vaccination against the flu virus may also reduce the risk of Alzheimer’s dementia for at least a few years ― adds to the already compelling reasons get the flu vaccine annually,” Avram Bukhbinder, MD, with McGovern Medical School at the UTHealth, Houston, Texas, told Medscape Medical News.
Sign me up.
Also from the public health front, Medscape tells us
About 80% of US adults have low to moderate cardiovascular (CV) health based on the American Heart Association (AHA) checklist for optimal heart health, which now includes healthy sleep as an essential component for heart health. With the addition of sleep, “Life’s Essential 8” replaces the AHA’s “Life’s Simple 7” checklist. * * *
The AHA Presidential Advisory — Life’s Essential 8: Updating and Enhancing the American Heart Association’s Construct on Cardiovascular Health — was published online June 29 in the journal Circulation.
A companion paper published simultaneously in Circulation reports the first study using Life’s Essential 8.
Overall, the results show that CV health of the US population is “suboptimal, and we see important differences across age and sociodemographic groups,” [Dr. Donald] Lloyd-Jones [chair of the department of preventive medicine at Northwestern University’s Feinberg School of Medicine in Chicago] said.
Medpage offers a detailed Q&A on monkeypox. Among them
Could monkeypox be spread easily from person to person, similar to COVID-19?
“Monkeypox is certainly not COVID-19,” stressed [Capt. Agam] Rao [, MD, a medical officer at the U.S. Public Health Service at the National Center for Emerging and Zoonotic Infectious Diseases (NCEZID)]. Based on prior outbreaks and the current outbreak, monkeypox appears to spread through “direct close contact. So, intimate contact that might happen during sex, but also any other close contact that might occur — for example, if you live with someone who has monkeypox and you are sleeping on the same bedding and using the same towels.”
“It really is not something that you will just pass on to someone walking down the street,” she said.
While agency researchers are “keeping an open mind” about the possibility that the virus could be more easily transmitted, “at this time, there’s no indication that it would spread the way that COVID spread and spread to as many people, [and] at this time, the risk for the worldwide population … is low,” she added.
From the prior authorization front, Healthcare Dive reports
Aetna is no longer requiring prior authorization for cataract surgeries, a controversial policy the payer adopted a year ago, according to a new provider notice.
Aetna is also rolling back prior authorization requirements for video EEGs and home infusion for some drugs. It’s adding two new-to-market drugs to the precertification list.
The payer said in a statement that it came to its decision after analyzing real-time data from the year the requirement was in place. “Going forward, we will focus on retrospective reviews of procedures and providers where questions of medical necessity exist,” Aetna said.
From the Rx coverage front, Fierce Pharma offers an article on how payers are planning to avoid cost shocks associated with gene therapy.
Kelley Miller, senior director of managed markets for the specialty pharmacy Optum Frontier Therapies, said there are three major considerations for his team during coverage talks. One is the clinical landscape, while another is the “human” element of what the patients and their families are going through. Thirdly, the team looks at the “economic impact” of the treatment.
Once Miller’s team has that information, the “conversations should come fast and furious,” he said.
Despite the biopharma industry’s advances in gene therapies, ICER president Steven Pearson, M.D., M.Sc., said it’s still a “fairly dicey business proposition” for companies in this field, especially outside the U.S. He pointed to bluebird bio’s decision to pull beta thalassemia gene therapy Zynteglo from the European market last year.
From the U.S. healthcare front, Beckers Hospital Review reports
IBM Watson Health, in partnership with Fortune, has released its top 15 health systems, which they find set an example for health systems and hospitals across the nation. With its data, the report will continue to stand as a resource for these groups to improve their quality of care and efficiency.
In its 14th year of publishing this study, IBM Watson Health found that the top 15 health systems had better survival rates, fewer patient complications, fewer healthcare-associated infections, better long-term outcomes, better 30-day mortality/revisitation rates and more. The study also found that patients revered the top 15 hospitals more than peer system hospitals.
For 2022, Allina Health of Minneapolis, MN, sits on top of the large health systems division. Cone Health of Greensboro, NC, sits on top of the medium health systems division. Asante of Medford Oregon sits on top of the small health system division.
From the Medicare Advantage front, Health Payer Intelligence discusses AHIP’s statement on the Medicare Advantage program which places various attacks against the MA program in perspective.
In addition to defending prior authorizations and spotlighting certain facets of OIG reporting, AHIP also offered evidence for Medicare Advantage plans’ efficacy overall.
The health plans have been proven to excel on quality measures and on overall efficiency, surpassing original Medicare’s quality level. They also have to ascribe to certain network adequacy standards.
Medicare Advantage plans produce savings for the Medicare program and offer higher value for members and taxpayers. In particular, Medicare Advantage plans offer strong value to members who are lower-income and underserved.
Lastly, AHIP pointed out that these plans have bipartisan support.
Finally federal employee benefits consultant Tammy Flanagan follows the retirement process of a federal employee in a three-part article in Govexec.
Note — Unfortunately, Thursday’s post did not arrive on the E&S website until 9 am ET today, so it did not go out to subscribers this morning. Lo siento. Here is a link to yesterday’s post.
Onto today’s post —
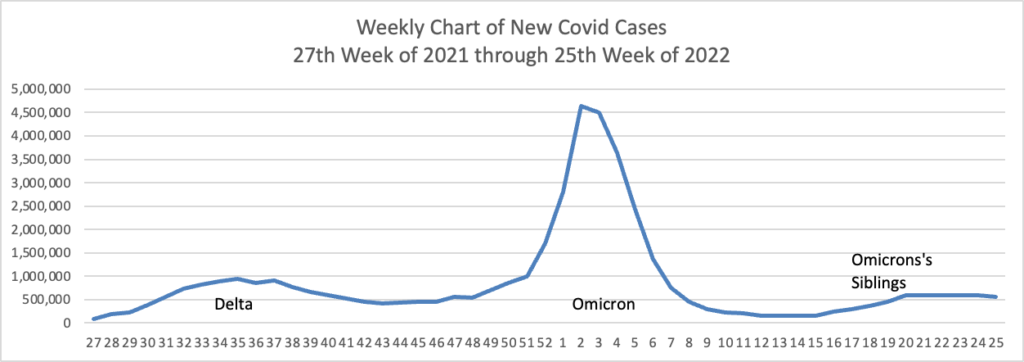
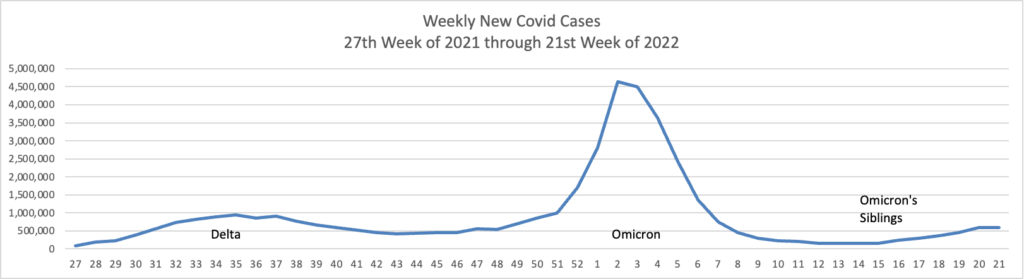
Based on the CDC’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s latest weekly chart of new Covid cases:
The CDC’s weekly review of its Covid statistics states “As of June 22, 2022, the current 7-day moving average of daily new cases (97,430) decreased 5.6% compared with the previous 7-day moving average (103,175).”
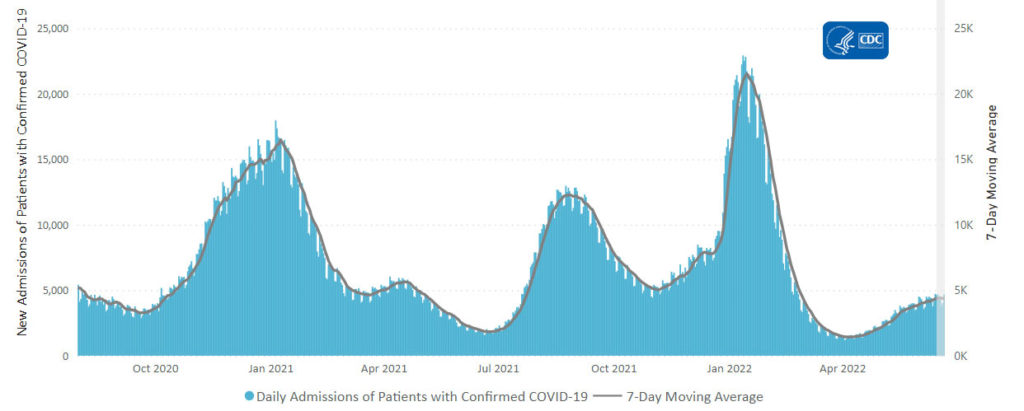
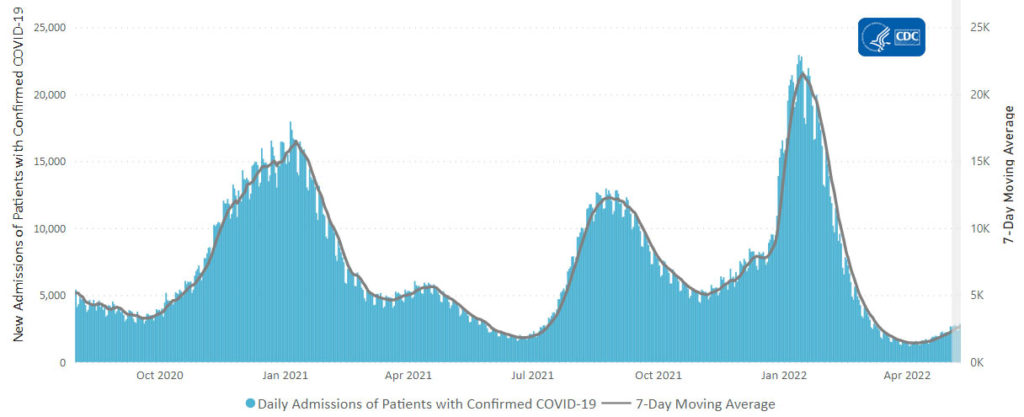
Here’s the CDC’s weekly chart of new Covid hospital admissions:
The CDC’s weekly review states “The current 7-day daily average for June 15–21, 2022, was 4,375. This is a 1.0% increase from the prior 7-day average (4,329) from June 8–14, 2022.”
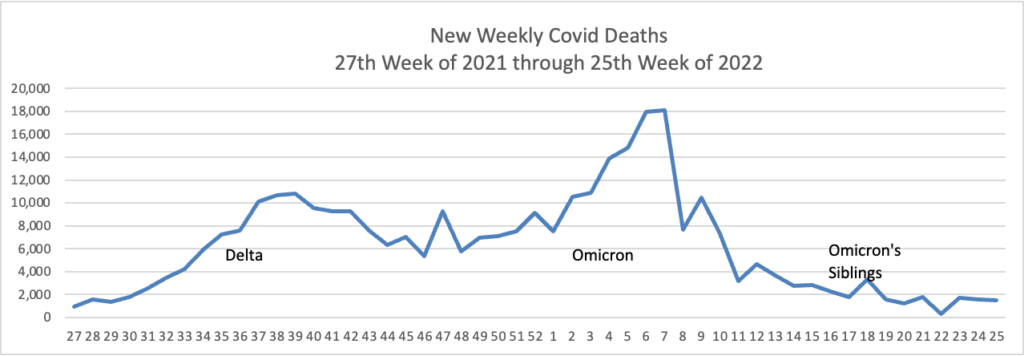
Here is the FEHBlog’s latest weekly chart of new Covid deaths:
The CDC’s weekly review states “The current 7-day moving average of new deaths (255) has decreased 10.4% compared with the previous 7-day moving average (285).”
As of June 23, 2022, there are 391 (12.1%) counties, districts, or territories with a high COVID-19 Community Level, 996 (30.9%) counties with a medium Community Level, and 1,830 (56.8%) counties with a low Community Level. This represents an increase (+1.9 percentage points) in the number of high-level counties, a slight increase (+1.6 percentage points) in the number of medium-level counties, and a corresponding decrease (−3.6 percentage points) in the number of low-level counties. 51 jurisdictions had high- or medium-level counties this week. Rhode Island is the only jurisdiction to have all counties at low Community Level.
The weekly statistics generally are stable and moving in the right direction.
The American Hospital Association adds
The Centers for Disease Control and Prevention last night endorsed Moderna’s COVID-19 vaccine for children aged 6-17, as its advisory committee recommended, creating an alternative to Pfizer’s COVID-19 vaccine for this age group. The Food and Drug Administration authorized the Moderna vaccine for children and adolescents last week.
Before ACA FAQ 50 issued October 4, 2021, the period for covering COVID vaccines with no cost sharing began 15 days after the CDC’s action. The FEHBlog, who is not errorless, thought that FAQ 50 eliminated the 15 day waiting period, but upon further review, FAQ 50 requires immediate no cost sharing coverage of Covid vaccines filing the FDA’s approval, usually an emergency use authorization. The FEHBlog doesn’t think this makes any practical difference because the Covid vaccines aren’t distributed without CDC approval.
From the Capitol Hill, the American Hospital Association provide us with this encouraging news:
The House of Representative today voted 234-193 to pass and send to the President for his signature bipartisan legislation to help reduce gun violence in communities. Approved by the Senate last night, the AHA-supported package includes behavioral health provisions, including funding for school safety resources, school-based supportive services and expanded access to telehealth for mental and behavioral health services.
From the Supreme Court, the Court decided today that the right to an abortion is a matter controlled by state law, not the U.S. Constitution. The Wall Street Journal sums it up as follows “In upholding a Mississippi law banning the procedure after 15 weeks of pregnancy, the court’s conservative majority said the Roe decision was egregiously wrong in recognizing a constitutional right to abortion.” In response
Reproductive health care, including access to birth control and safe and legal abortion care, is an essential part of your health and well-being. While Roe v. Wade was overturned, abortion remains legal in many states, and other reproductive health care services remain protected by law. The U.S. Department of Health and Human Services (HHS) is committed to providing you with accurate and up-to-date information about access to and coverage of reproductive health care and resources. Our goal is to make sure you have appropriate information and support.
Health Payer Intelligence discusses health insurer reaction to the decision. “Payers and healthcare leaders are responding to the Supreme Court’s decision to overturn Roe v Wade, the case which protected abortion rights at the federal level, and while the repercussions remain uncertain many healthcare leaders are voicing their commitment to helping women navigate the impacts.”
The Wall Street Journal discusses employer reaction to the decision. “Businesses with health plans covering abortion now are weighing whether and how to pay for employees to travel to a state where the procedure is legal.”
From the OPM front
Federal News Network reports on OPM Director Karen Ahuja’s press conference held yesterday, the first anniversary of her swearing in as OPM Director.
FedWeek tells us that “OPM has said it is working to improve features for federal employees and annuitants to compare FEHB plans, although it does not project having those improvements in place until late next year—potentially in time for that year’s open season for selecting coverage in 2024.”
From the nicotine front, the Wall Street Journal reports
A federal appeals court on Friday granted Juul Labs Inc. a temporary stay of the Food and Drug Administration’s order for the vaping company to pull its e-cigarettes off the U.S. market.
A panel of judges from the U.S. Court of Appeals for the D.C. Circuit on Friday afternoon granted Juul’s request to delay the FDA’s ban, according to court documents. The temporary stay gives the court time to hear arguments and wasn’t a ruling on the merits of the case, the judges wrote.
Finally, HR Dive brings us a roundup of happenings at this week’s Society for Human Resource Management conference.
The Senate on Thursday took a major step toward broadening America’s commitment to take care of sick veterans, passing a bill to offer new health care and tax-free disability benefits to as many as 3.5 million veterans on an 84-14 vote.
Under the legislation written by Veterans’ Affairs Chairman Jon Tester, D-Mont., and ranking member Jerry Moran, R-Kan., the Department of Veterans Affairs would consider a veteran with any of 23 conditions, ranging from brain cancer to hypertension, who was deployed to a combat zone during the wars in Iraq or in Afghanistan automatically eligible for care at government cost, based on the presumption that exposure to toxic chemicals in the war zone caused the ailments.
The House must now pass the revised bill before President Joe Biden can sign it, which seems likely. The legislation largely mirrors, and slightly expands on, a House bill by Veterans’ Affairs Chairman Mark Takano, D-Calif., that passed 256-174 in March. Biden issued a statement at the time saying he supported the measure.
Under current law, veterans who believe toxic exposure during their service caused them to develop a disease can have trouble proving it, even when the linkage is known. So it’s likely that many veterans are denied care and disability benefits they deserve, advocates say. The new law, at a projected cost of $278.5 billion over 10 years, shifts the calculus, meaning the government will now pay for the care of veterans whose sickness is tied to their service, as well as others whose ailments might not be.
Because the federal government employs many veterans, this bill will reduce benefits costs for the FEHB Program once it becomes law.
From the Omicron and siblings front, the Wall Street Journal informs us
Many people are embarking on a summer of vacations, concerts and weddings put off during the height of the pandemic. Covid-19 is still finding ways to disrupt some of those plans.
Covid-19 isn’t causing acute illness and death on the scale it once did, thanks in part to protection built up by vaccines and prior infections. * * *
The U.S. is logging some 100,000 known cases a day, and many more are being detected via at-home tests health departments don’t track. This is a stark difference from a year ago, when U.S. cases sank below 12,000 a day, the lowest level since the first surge, as vaccinations rose and many hoped the virus was in retreat.
The era of 12,000 cases a day was over when Delta and then Omicron arrived and will remain around until Omicron departs.
In a notable move, the Federal Trade Commission put drugmakers and pharmacy benefit managers on notice that the agency will “ramp up enforcement” of any “illegal bribes and rebate schemes” that make it harder for patients to access lower-cost medicines.
The new policy statement noted the FTC plans to scrutinize rebates and assorted fees for signs that these payments are violating antitrust and consumer protection laws. As part of that effort, the agency expects to monitor lawsuits and file its own legal briefs in cases where it can provide assistance in analyzing illegal practices that may raise prescription drug prices.
“Today’s action should put the entire prescription drug industry on notice: when we see illegal rebate practices that foreclose competition and raise prescription drug costs for families, we won’t hesitate to bring our full authorities to bear,” said FTC Chair Lina Khan in a statement. “Protecting Americans from unlawful business practices that are raising drug prices is a top priority for the Commission.”
While the end of Omicron is not in the offing, the end of prescription drug rebates appears to be getting closer. However, the federal government should not put the kibosh on rebates unless the drug manufacturers agree to maintain the economic equities by offering price reductions equivalent to the rebates.
Drugmaker acquisitions of all sizes could receive closer scrutiny in the future if the Federal Trade Commission follows the advice of experts who spoke at a two-day agency meeting on market concentration and anticompetitive conduct.
The experts, mostly economists and other antitrust regulators, warned that some drugmakers have gained unfair market power due to the breadth of their product portfolios, allowing them to negotiate for preferred or even exclusive status on insurers’ coverage lists and thereby squeeze out competitors.
Taken together with the FTC’s plans to investigate the practices of pharmacy benefit managers, the meeting signals the Biden administration may take a tougher line on monopolistic practices in an effort to spark competition and target drug pricing.
From the Food and Drug Administration front, BioPharma Dive notes that
An experimental and closely followed drug for Alzheimer’s disease has failed a key clinical study, dealing yet another blow to the prevailing theory on how to treat a neurodegenerative illness that affects millions of people.
The drug’s developer, Roche, along with Banner Alzheimer’s Institute, the Phoenix-based organization helping lead the study, announced the negative results Thursday. After years following a family believed to be genetically predisposed to the disease, researchers found no significant difference in cognition or the ability to store and retrieve new memories between participants who received the drug and those who got placebo.
The failure is an upset not only to Roche, which hopes to follow its rival Biogen in getting an Alzheimer’s therapy approved for market, but also to the wider Alzheimer’s research field. For years, a protein called beta amyloid has been at the center of efforts to treat the disease. But every drug designed to block this protein, including Biogen’s, has faced setbacks. Roche’s announcement may therefore add to concerns that this protein isn’t the best research target.
In other drug research news, Walgreens announced “the launch of its clinical trial business to redefine the patient experience and increase access and retention in sponsor-led drug development research. Walgreen’s flexible clinical trial model combines the company’s vast foundation of patient insights, partner-enabled health and technology capabilities and in-person and virtual care options to break through barriers to engaging broader and more diverse communities.”
In U.S healthcare news, the American Medical Association completed its annual meeting. The AMA offers highlights from the session here.
Also, the Commonwealth Fund released its 2022 Scorecard on State Health System Performance.
Hawaii and Massachusetts top the 2022 State Scorecard rankings, based on overall performance across 56 measures of health care access and quality, service use and cost, health disparities, and health outcomes during the COVID-19 pandemic in 2020. The lowest-performing states were Mississippi, Oklahoma, and West Virginia.
From 2000-2019 overall life expectancy in the United States increased by 2.3 years, but the increase was not consistent among racial and ethnic groups and by geographic area. In addition, most of these gains were prior to 2010. This is according to a new study funded by the National Institutes of Health that examined trends in life expectancy at the county level. The study was led by researchers at the Institute for Health Metrics and Evaluation at the University of Washington’s School of Medicine, Seattle, in collaboration with researchers from NIH and published on June 16th in The Lancet.
MedCity News reports “Online healthcare marketplace Sesame closed a $27 million Series B funding round on Tuesday, bringing its total funding to $75 million. David Goldhill, CEO of the New York City-based startup, said the company is ‘an Expedia for medical care’ because patients can buy the care they want directly online, without the middleman of an insurance company.”
From the federal employee benefits front, Govexec delves into the impact of cost of living adjustments on federal employee retirement benefits.
From Capitol Hill, Medpage Today suggests that prior authorization practices are under Congress’s spotlight.
From the Omicron and siblings front–
The Wall Street Journal offers an interesting report on the ups and downs of Omicron and its siblings.
Govexec tells us about recent Safer Federal Workforce changes to “its COVID-19 protocols to draw more distinctions between the policies for vaccinated and unvaccinated workers, including those related to travel and paid leave.”
From the federal employment front, the Society for Human Resource Management explains how the federal government is “struggling mightily to recruit, retain and develop the talent it needs to succeed and earn the reputation of being a “model employer.” Agencies and their HR leaders are working to upgrade antiquated systems and processes. The new-hire process currently takes an average of 100 days to complete, double that of the private sector.” Good luck.
From the Rx coverage front, Prime Therapeutics announced last week
Leading pharmacy benefit manager (PBM) Prime Therapeutics LLC (Prime) analyzed its real-world data to assess clinical outcomes and drug waste differences between medically integrated dispensing (MID) and central specialty pharmacy dispensing of oral cancer therapies. This study of a Prime pilot program showed a potential average savings opportunity of $1,800 per medication dose change at a MID pharmacy compared to a central fill specialty pharmacy. Results reinforced Prime’s position of the advantages of the MID model, on which its IntegratedRx™ program is based.
With the MID model, care providers – including doctors and pharmacists – have access to prescribing history, test results and other important patient information in the EMR. This coordination informs the care team earlier than the traditional model. This early look has potential to help lower the number of 30-day prescriptions going to waste.
Prime’s MID pilot program was implemented in early 2021 within three oncology practices and across three Blue Plans’ commercially insured lives to prove the potential care and cost advantages with this distinct model compared to a centralized specialty pharmacy model. Study participants were prescribed oral drugs that did not require dispensing and shipment from a payer-directed specialty pharmacy to the oncologist (aka white bagging).
From the studies department —
Health Payer Intelligence informs us “More consumers reported that their health plans are offering transparency tools and overall consumer awareness about the availability of transparency tools has grown, according to a study conducted on behalf of HealthSparq.”
MedPage Today discusses a study finding that weight loss, even when achieved by bariatric surgery, will reduce the risk of obesity-related cancer. The FEHBlog wonders if weight loss produced by the current, effective weight loss drugs would have a similar health impact.
mHealth Intelligence notes that “To reduce the amount of time spent in a virtual waiting room, researchers from the University of California San Diego conducted a pilot that used text messaging to provide patients with a meeting link when their provider was ready to see them, finding it to be a successful alternative.”
The New York Times reports on a GlaxoSmithKline “checkpoint inhibitor” drug trial conducted on eighteen rectal cancer patients. The drug wiped out the cancer in all of those patients. Quite amazing. According to the Times experts indicate that the trial needs to be replicated.
BioPharma Dive reports “Twenty-four years ago, a drug called Herceptin changed how doctors treat breast cancer. Its approval in 1998 made it possible to target the aggressive breast tumors tied to a gene called HER2. Other drugs quickly followed Herceptin and, over the years since, have substantially improved survival for people with the disease. A quarter of a century later, another shift in treatment could be on the horizon. At the American Society of Clinical Oncology meeting, AstraZeneca and Daiichi Sankyo are presenting results proving that, for the first time, a targeted medicine can help metastatic breast cancer patients whose tumors express only low levels of HER2. Clinical trial data revealed at ASCO and published in The New England Journal of Medicine Sunday show the drug, Enhertu, halved the risk of cancer progression compared to chemotherapy and reduced the risk of death by 36%.”
The Guardian tells us “Taller people have an increased risk of peripheral neuropathy, as well as skin and bone infections, but a lower risk of heart disease, high blood pressure and high cholesterol, according to the world’s largest study of height and disease. A person’s height raises and reduces their risk of a variety of diseases, according to the research led by Sridharan Raghavan of the Rocky Mountain Regional VA Medical Center in the US. The findings are published in the journal PLOS Genetics.”
From the potpourri department, check out this NIH Newsletter for June 2022.
From Washington, D.C., and “Following a meeting of the Social Security and Medicare Boards of Trustees, the U.S. Department of the Treasury—joined by Departments of Health and Human Services and Labor, the Centers for Medicare & Medicaid Services, and the Social Security Administration—released the annual Social Security and Medicare Trustees Reports.” Here is a link to the government’s fact sheet on those reports.
The American Hospital Association explains
The Medicare Hospital Insurance Trust Fund will have sufficient funds to pay full benefits until 2028, according to the latest annual report released today by the Medicare Board of Trustees.
That’s two years later than last year’s report. The HI Fund, known as Medicare Part A, helps pay for inpatient hospital services, hospice care, and skilled nursing facility and home health services following hospital stays.
HI income is projected to be higher than last year’s estimates because both the number of covered workers and average wages are projected to be higher, according to the report. In addition, HI expenditures are projected to be lower than last year’s estimates in the beginning of the short-range period mainly due to the pandemic but are projected to become larger after 2023 due to higher projected provider payment updates.
“There is substantial uncertainty in the economic, demographic, and health care projection factors for HI trust fund expenditures and revenues,” the report notes. “Accordingly, the date of HI trust fund depletion could differ substantially in either direction from the 2028 intermediate estimate.”
More than two-thirds of the world’s population probably have significant levels of Covid-19 antibodies, meaning they have either been infected or were vaccinated, the World Health Organization said.
So-called seroprevalence rates surged to 67% in October from 16% in February of 2021, the WHO said, in a summary of studies from around the globe. Given the emergence of the fast-spreading omicron variant, the figure is probably even higher now.
A large randomized, placebo-controlled clinical trial led by the National Institutes of Health shows that treating adults hospitalized with COVID-19 with infliximab or abatacept – drugs widely used to treat certain autoimmune diseases – did not significantly shorten time to recovery but did substantially improve clinical status and reduce deaths.
That’s a good trade-off.
From the federal employee benefits front
OPM released a proposed Federal Long Term Care Insurance Program rule today. The rule indicates that OPM is planning a suspension of enrollments in this Program. “For example, it may be appropriate to suspend applications to allow a period of time for revisions to underwriting processes or for premium repricing after a review of actuarial assumptions, in order to ensure that premium rates reasonably and equitably reflect the cost of the benefits provided as required by the statute and to ensure that OPM can provide eligible individuals with the information needed to enable them to fully evaluate the advantages and disadvantages of obtaining LTCI under FLTCIP.” (pp. 4-5). The public comment deadline is expected to be July 2, 2022.
Benefits consultant Tammy Flanagan responds in Govexec to reader questions about “about choosing when to retire in order to maximize the impact of both the annual cost-of-living adjustment to retirement benefits and the yearly federal employee pay increase.” Check it out.
From the transparency front
Roll Call discusses the progress of the hospital industry in achieving compliance with the federal government’s pricing transparency rule which became enforceable eighteen months ago.
While most hospitals have been willing to follow parts of the rule — namely, a requirement that they post user-friendly lists or tools to help patients shop for services — they have been less compliant with a requirement that they post “machine readable” files of standard charges — data that experts say would be far more useful in driving down costs.
That’s an intriguing factoid because the federal government’s health plan transparency rule’s similar requirement to post three “machine readable” files of claim payments data becomes enforceable on July 1, 2022.
From the Rx coverage front, Healthcare Dive informs us
* Rite Aid is the latest pharmacy giant to step into clinical care delivery through a new partnership with rural home care startup Homeward.
* Under the deal announced Tuesday, Rite Aid pharmacists will direct eligible customers to Homeward’s clinical services, including annual wellness visits, health screenings, diagnostic testing, virtual visits and in-home care. Homeward will also be able to park its mobile clinician units at Rite Aid’s rural locations, with the goal of allowing senior customers to see a provider and pick up their prescriptions in one visit.
* Homeward will provide in-network services, including specialty care beginning with cardiology, in the third quarter this year for patients covered by Medicare and Medicare Advantage plans. The companies are starting the partnership in Michigan, with the opportunity to expand to Rite Aid’s 700 rural locations across the U.S. over time.
Based on the CDC’s Covid Data Tracker, and using Thursday as the first day of the week, here is the FEHBlog’s weekly chart of new Covid cases from the 27th week of 2021 through the 21st week of 2022:
Reliable estimates of case counts are particularly relevant with the U.S. in the midst of yet another Covid-19 wave. By official case counts, it is a modest wave, at roughly 110,000 infections a day, according to the CDC. That is smaller than the 165,000 daily cases reported during the Delta wave, or the 250,000 a day during the 2020-21 winter.
But estimates of the true number of infections, correcting for undercounting, suggest the U.S. might be experiencing the second-largest wave of Covid-19 infections since the pandemic began.
Here’s the CDC’s weekly chart of new Covid hospitalizations.
Hospitalization numbers also aren’t a perfect gauge. Someone can break a leg and test positive in the emergency room for a mild case of Covid-19. That case becomes a confirmed coronavirus hospitalization—and a strain on the hospital’s bed counts and personal-protective-equipment supplies—but not necessarily a severe case.
In Massachusetts, hospitals have begun reporting whether Covid-19 is the primary reason someone is in the hospital—and in January about 50% of cases were. It is hard to pinpoint how similar Massachusetts would be to other states, but it offers a further example of how better counting could improve assessment of the pandemic.
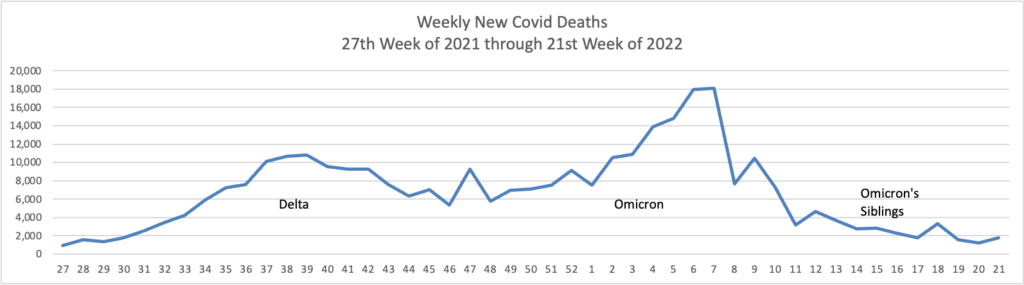
Here’s the FEHBlog weekly chart of new Covid deaths again from the 27th week of 2021 through the 21st week of 2022:
Covid-19 deaths in the U.S. are hovering near the lowest levels since the pandemic hit, showing how a population with built-up immune protection is less at risk of severe outcomes even as another wave of infections flows through the country.
The nearly 300 deaths reported daily are again more concentrated among older people, underscoring hazards for the more vulnerable while the overall population appears less at risk.
Particularly vulnerable people, such as those who are older and immunocompromised, will likely always have some risk of death from a Covid-19 infection, doctors and public-health experts said. Increasing booster rates and access to treatments, in addition to taking certain precautions, can help lower the threat presented by the virus, they said.
White House officials said on Thursday that they were introducing new models for distributing Paxlovid, the Covid-19 oral medication made by Pfizer, in an effort to get the treatment to more people and keep coronavirus death rates relatively low even as cases increase.
The federal government will start reimbursing a clinic in Providence, R.I., for evaluating patients who test positive and immediately prescribing Paxlovid to those eligible for it — the first of what the White House said would be a series of federally supported sites, with others set to open in New York and Illinois. Federal workers are also being sent to state-run testing sites in Minnesota, transforming them into “test-to-treat” locations, the White House said.
“Fundamentally, what we’re trying to do is get to a point where Covid deaths are largely preventable, and I think we’re pretty close to there,” Dr. Ashish K. Jha, the White House Covid-19 response coordinator, said in an interview Wednesday evening. “Deaths from this disease really should become increasingly rare.”
STAT News offers an interesting look into how scientists assess the level of Covid resistance to Paxlovid.
Resistance is the hobgoblin of antiviral medicine, even with antivirals as effective as Paxlovid. After doctors deployed nearly every new virus-killing infusion or pill in history, strains popped up — either immediately or eventually — with machinery warped in just the right way to evade the threat.
Exactly how much of a problem resistance will be for Paxlovid is complicated. In some patients, the coronavirus will inevitably find ways to evade the pill, as it did prior Covid-19 drugs.
“If there is anything we know about viruses and antiviral drugs is that eventually we will see some sort of resistance,” Andrew Pavia, chief of pediatric infectious diseases at University of Utah Health, said in an email.
What’s less clear, Pavia and other experts say, is whether any resistant variants will spread widely. The coronavirus may have particular difficulty getting around Paxlovid compared to other drugs because patients take it for only five days and because it targets a protein the virus can’t easily change. Any mutation or modification the virus makes may impair its ability to replicate or survive.
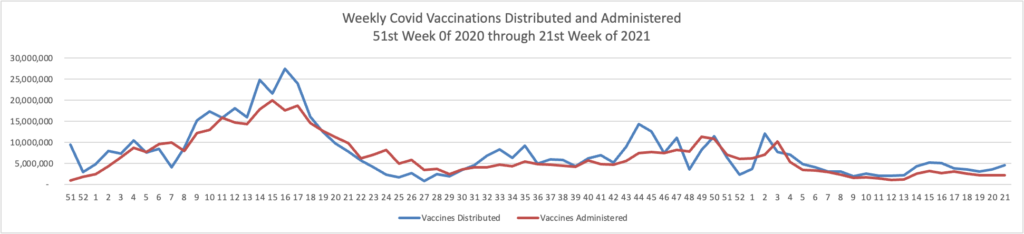
Here’s the FEHBlog weekly chart of Covid vaccinations distributed and administered
The CDC’s weekly review of its Covid statistic tells us
People who are up to date on vaccines have much lower risk of serious illness and death from COVID-19 compared with people who are unvaccinated. CDC’s COVID Data Tracker shows that in March 2022, adults ages 18 years and older who were unvaccinated were about 5 times more likely to be hospitalized with COVID-19 than those who were up to date. In the same month, people ages 12 years and older and unvaccinated were 17 timesmore likely to die of COVID-19 than those who were up to date.
COVID-19 vaccines available in the United States are effective at protecting people from getting seriously ill, being hospitalized, and even dying—especially people who are boosted. As with other diseases, you are protected best from COVID-19 when you stay up to date with recommended vaccines. Find a vaccine provider near you.
As of May 19, 2022, there are 301 (9.35%) counties, districts, or territories with a high COVID-19 Community Level, 477 (14.81%) counties with a medium Community Level, and 2,442 (75.84%) counties with a low Community Level. This represents a moderate (+5.10 percentage points) increase in the number of high-level counties, a slight (−0.74 percentage points) decrease in the number of medium-level counties, and a corresponding (−5.84 percentage points) decrease in the number of low-level counties. Five (9.62%) of 52 jurisdictions had no high- or medium-level counties this week.
the Centers for Medicare & Medicaid Services (CMS) released a report that recommends cost savings from lower-than-expected Medicare Part B spending be passed along to people with Medicare Part B coverage in the calculation of the 2023 Part B premium. Earlier this year, Department of Health and Human Services (HHS) Secretary Xavier Becerra instructed CMS to reassess the 2022 Part B premium amount in response to a price reduction for Aduhelm™, a monoclonal antibody directed against amyloid for use in treating Alzheimer’s disease. Given the information available today, it is expected that the 2023 premium will be lower than 2022. The final determination will be made later this fall.
This CMS decision is quite sensible, in the FEHBlog’s view.
On a related FEHB note, FedSmith discusses the pros and cons of enrolling in Medicare Part B when you are a federal or Postal annuitant with FEHB coverage in retirement as well.
From the telehealth front, mHealth Intelligence reports
Called CVS Health Virtual Primary Care, the digital care platform will provide healthcare consumers with an array of care services, including primary care, on-demand care, chronic condition management, and mental health services. Consumers will also be able to choose their healthcare setting from various retail, community-based, virtual, and at-home care options.
“We’re meeting people where they are on their healthcare journey and providing care that is more convenient and easier to access,” said Creagh Milford, DO, vice president, enterprise virtual care at CVS Health, in the news release.
The new benefit will launch on January 1, 2023.
From the Rx coverage front, Formulary Watch reveals that
The Institute for Clinical and Economic Review (ICER) has released the protocol for its second annual review of insurance company policies to assess fair access to prescription drugs. ICER will evaluate whether 15 large U.S. commercial payers, the two largest state health exchange plans, and the Department of Veterans Affairs have formularies and procedures that provide appropriate access to the prescription drugs reviewed by ICER in 2020. These drugs include those that treat patients with cystic fibrosis, hemophilia A, migraine, sickle cell disease, and ulcerative colitis.
The analysis is expected to be completed in November 2022.
From the studies front, the Centers for Disease Control issued its 2021 Diabetes Report Card this week. Here are the highlights
* After almost 2 decades of continual increases, the incidence of newly diagnosed cases of diabetes in the United States decreased from 9.3 per 1,000 adults in 2009 to 5.9 per 1,000 adults in 2019.
* Prevalence of prediabetes among US adults remained steady from 2005–2008 to 2017–2020. However, notification of prediabetes status nearly tripled (from 6.5% to 17.4%).
* American Indian or Alaska Native, non-Hispanic Black, Hispanic, and non-Hispanic Asian people are more likely to be diagnosed with diabetes than non-Hispanic White people (14.5%, 12.1%, 11.8%, 9.5%, and 7.4%, respectively).
* During the COVID-19 pandemic, diabetes emerged as an underlying condition that increases the chance of severe illness. Nearly 4 in 10 adults who died from COVID-19 in the United States also had diabetes.
Lawmakers are facing increased pressure to pass a comprehensive mental health and substance use package but are unlikely to make an initial goal of advancing legislation before the implementation of a three-digit suicide hotline in July.
At least four congressional committees have committed to advancing a swath of bipartisan mental health bills under their jurisdiction, but lawmakers have not yet unlocked the puzzle of how to incorporate a growing laundry list of programs to authorize and establish existing and new programs dedicated to treatment, prevention, education, crisis care, drug interdiction and the workforce.
One of those four committees is the Senate Finance Committee which announced today
Senate Finance Committee Chair Ron Wyden (D-Ore.), Ranking Member Mike Crapo (R-Idaho), Senator Ben Cardin (D-Md.) and Senator John Thune (R-S.D.) today released a discussion draft for telehealth policies as a part of the committee’s ongoing work to improve mental health care across the nation, which has included a public call for comments and three hearings to help develop these initiatives. * * *
The discussion draft includes policies that would:
* Remove Medicare’s in-person visit requirement for tele-mental health services.
* Establish benefit transparency for mental health care services delivered via telehealth to inform Americans with Medicare how and when they can access telehealth.
* Preserve access to audio-only mental health coverage in Medicare when necessary and appropriate.
* Direct Medicare and Medicaid to promote and support provider use of telehealth.
* Incentivize states to use their CHIP programs to establish local solutions to serve behavioral health needs in schools, including through telehealth.
A highly contagious sublineage of the BA.2 omicron subvariant is now the nation’s dominant strain, according to the CDC’s latest variant proportion estimates.
The sublineage, BA.2.12.1, accounted for 57.9 percent of all U.S. COVID-19 cases in the week ending May 21, CDC data shows. BA.2, which became the nation’s dominant strain in mid-March, now accounts for an estimated 39.1 percent of all cases.
BA.2.12.1 is estimated to have a 25 percent growth advantage over BA.2, which is already more transmissible than the original omicron strain. The newer omicron sublineage has been gaining traction in the U.S. over the last month. In the week ending April 23, BA.2.12.1 accounted for just 24.1 percent of U.S. COVID-19 cases.
Health officials are also monitoring another omicron subvariant — BA.1.1.529 — which currently accounts for an estimated 2.8 percent of cases.
“Epidemiologically, it doesn’t appear as if we’re seeing more severe disease in places that are having more cases,” CDC Director Rochelle Walensky said of the sublineages during an April 26 news conference. “So we are not anticipating more severe disease from some of these subvariants, but we are actively studying it.”
As many as one in four seniors and one in five adults under 65 experienced “long COVID” or “post-COVID” symptoms after surviving a coronavirus infection, a new study from the Centers for Disease Control and Prevention reported Tuesday.
The study — published in the CDC’s Morbidity and Mortality Weekly Report — is the latest to try and quantify how many of the millions of Americans who have now tested positive for the virus are facing long-term issues caused by their infection.
By comparing electronic health records in a large national database of patients, the study’s authors found 38.2% of COVID-19 survivors “experienced at least one incident condition” — a list that includes heart, lung, kidney and gastrointestinal problems, pain, fatigue, loss of smell or taste, mental health issues, and more — in the months after their infection. By contrast, just 16% of other people were diagnosed with such conditions.
Vaccination reduces your risk of developing long Covid, but not by much on average, new research suggests.
A Veterans Affairs study out Wednesday found that vaccinated people with breakthrough Covid-19 infections had a 15% reduction in experiencing persistent or new symptoms and health conditions up tosix months after infection compared with those who were unvaccinated and got Covid.
Most of the vaccinated people had received two doses of the Pfizer or Moderna vaccine, while 8% received one dose of the Johnson & Johnson vaccine.The study didn’t look at people who had received boosters.
Bloomberg discusses the risks of contracting Covid while pregnant.
Canada’s first dual specialist in infectious diseases and obstetrics/gynecology, Deborah Money, MD comments “For the most part, women in communities even with Covid circulating do well,” she says. “The majority of babies are fine.”
But that’s just part of the story. Their analysis of data from 6,012 people in six Canadian provinces who tested positive for the virus during their pregnancy found a substantial increase in hospitalizations and ICU admissions compared with reproductive-age, non-pregnant females infected with the coronavirus. Their study in the May 2 issue of the JAMA medical journal also found that 11.1% of Covid–affected pregnancies resulted in preterm birth, compared with 6.8% among all unaffected Canadian pregnancies. * * *
Money says it underscores the need for obstetricians to carefully monitor their pregnant patients who become infected with SARS-CoV-2, and for expecting moms to get vaccinated and boosted.
“That’s the biggest thing they can do,” she says. “It really does look like vaccine is preventative for the serious outcomes.”
From the studies front —
The Medical Group Management Association informs us “Despite multiple waves of disruption in 2021, medical practices navigated through the “new normal” of COVID-19 to restore a sense of normalcy in productivity and compensation last year.”
Milliman released its 2022 Medical Index (MMI). “In 2022, the cost of healthcare for a hypothetical American family of four covered by an average employer sponsored PPO plan is $30,260,” 4.6% above 2021.
HR Dive tells us “[a] 2019 IRS notice expanded the list of medications and health services Health Savings Account-eligible health plans may cover prior to meeting a patient’s deductible. Employers that take advantage of the expansion could cover these treatments with little to no increases in patient premiums, according to an Employee Benefits Research Institute report published May 19.”
Commercial insurance members’ satisfaction with their plans stayed flat between 2021 and 2022, according to a new survey from J.D. Power.
Satisfaction was on a steady climb over the past five years, the survey found, but plateaued in the past year amid declines in how well members’ expectations for customer service were met and dissatisfaction with their plan designs and network providers.
Health plans that were perceived by members as responsive enjoyed higher scores than those that were not, J.D. Power found. The Kaiser Foundation Health Plan and regional Blues insurers were consistently ranked as the highest scoring in the study’s 22 geographic regions.
From the mental healthcare front, the International Foundation of Employee Benefit Plans notes
The U.S. Department of Labor (DOL) published new guidance on obtaining job protected leave under the Family and Medical Leave Act (FMLA) for workers seeking mental health support. The guidance clarifies that eligible employees are able to take FMLA leave for their own serious health condition or to care for a spouse, child or parent because of their serious health condition, and that a serious health condition can include a mental health condition.
From the federal employee benefits front, benefits consultant Tammy Flanagan writes in Govexec about Federal Employee Group Life Insurance Program options for federal and postal annuitants. What’s more, Fedweek explains how FEHBP fills Medicare coverage gaps for those fine folks.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.