Friday Stats and More
Happy Lincoln’s Birthday.
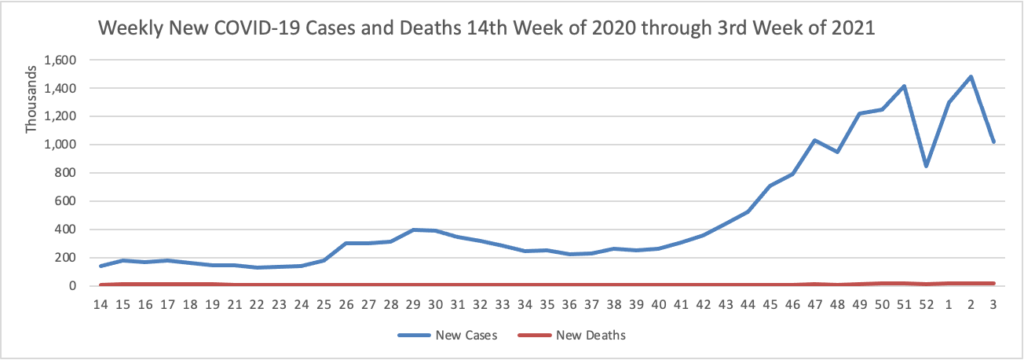
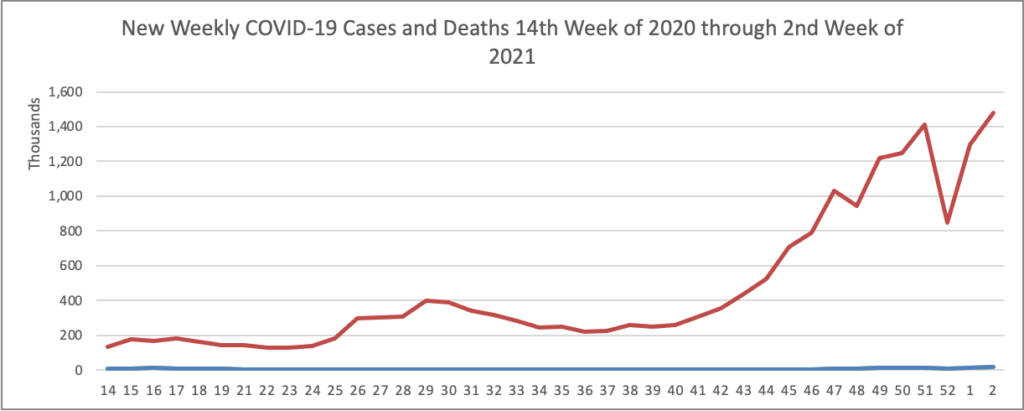
Based on the Centers for Disease Control’s COVID-19 Case Tracker website, here is the FEHBlog’s chart of new weekly COVID-19 cases and deaths over the 14th week of 2020 through the 6th week of this year (beginning April 2, 2021, and ending February 10, 2021; using Thursday as the first day of the week in order to facilitate this weekly update):

and here is the CDC’s latest overall weekly hospitalization rate chart for COVID-19:

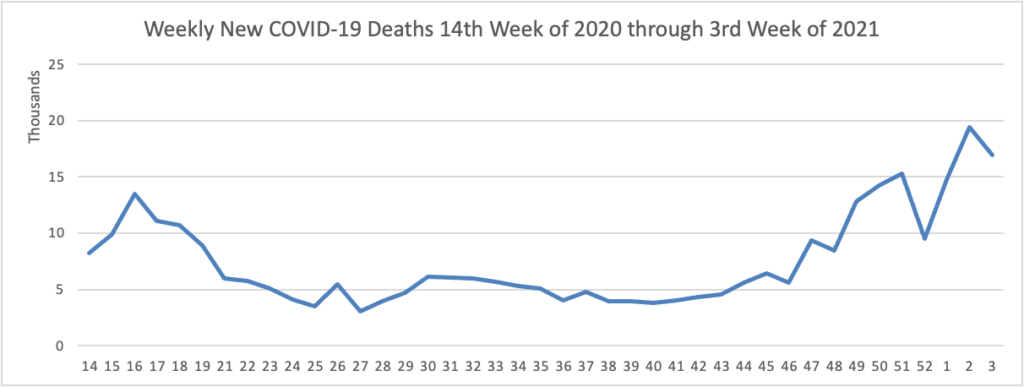
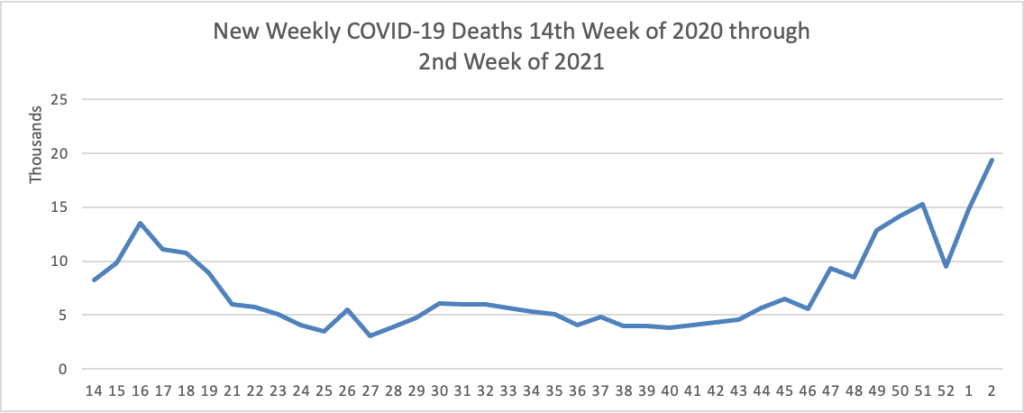
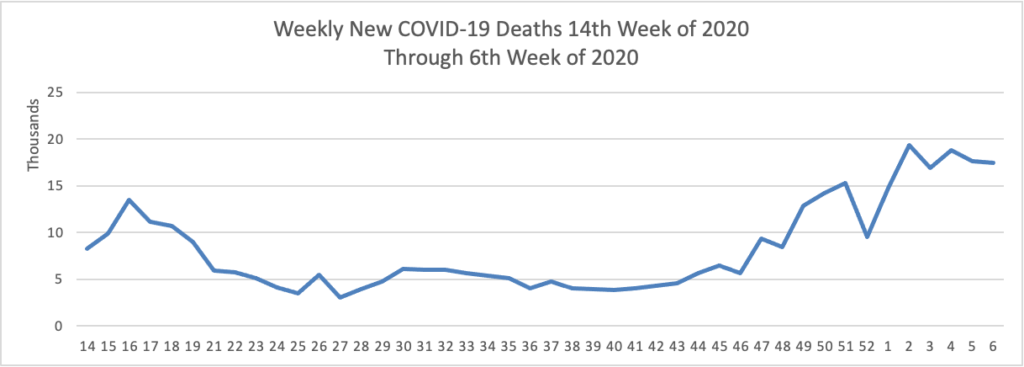
The FEHBlog has noticed that the new cases and deaths chart shows a flat line for new weekly deaths because new cases greatly exceed new deaths. Accordingly here is a chart of new weekly COVID-19 deaths over the period April 2, 2020, through February 10, 2021):
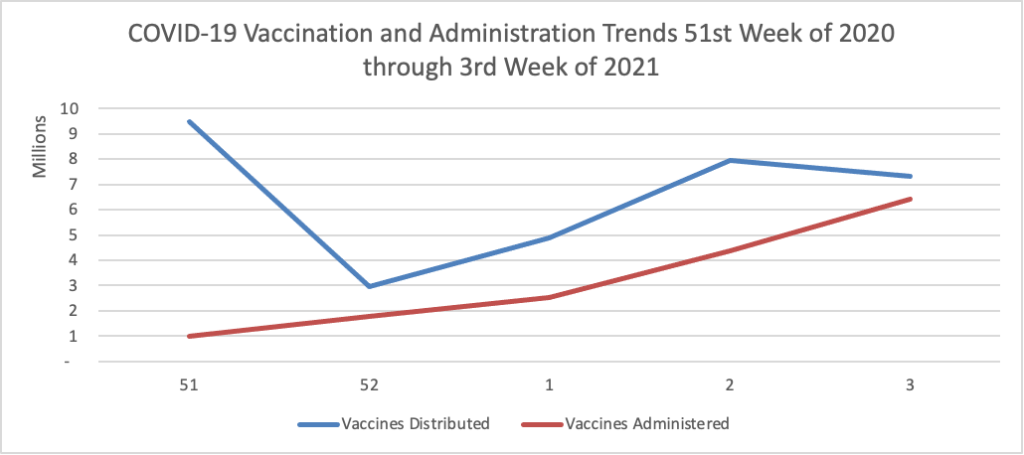
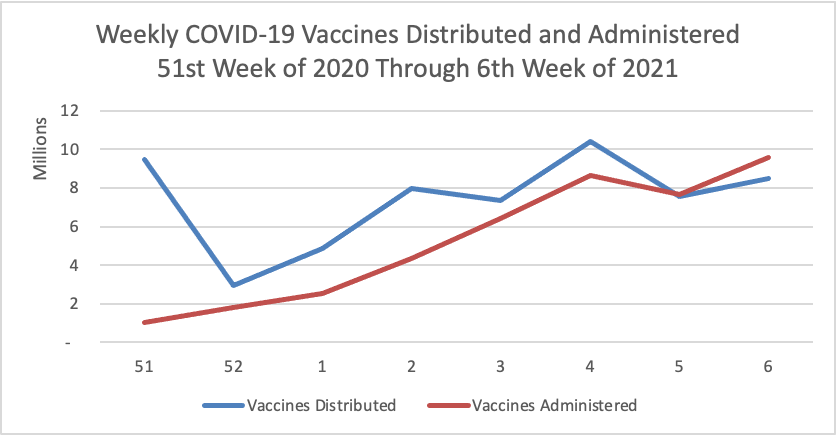
Finally here is a COVID-19 vaccinations chart from December 17, 2020, through February 10, 2021, which also uses Thursday as the first day of the week:
The Wall Street Journal sums it up well for this week :
U.S. Covid-19 deaths [a lagging indicator] appear to finally be slowing, following a broad and steep decline in both newly reported cases and hospitalizations in recent weeks.
While daily deaths remain near record highs, the average number of coronavirus-related fatalities has broadly fallen in recent days, dropping from a seven-day average of 3,172 on Feb. 1 to 2,765 on Wednesday, according to a Wall Street Journal analysis of Johns Hopkins University data.
Vaccinations, meanwhile, appear to be increasing, with about two million shots administered Thursday, according to a Wall Street Journal analysis of data from the Centers for Disease Control and Prevention.
In other vaccination news —
- Medpage Today informs us about CDC changes to its adult and children vaccination recommendations which were released yesterday.
- HR Dive reports that
The Society for Human Resource Management and 41 other business groups including the U.S. Chamber of Commerce have asked the U.S. Equal Employment Opportunity Commission (EEOC) to clarify “the extent to which employers may offer employees incentives to vaccinate.”
In a Feb. 1 letter to EEOC Chair Charlotte Burrows HR Dive obtained from the HR Policy Association, a signee, the groups wrote that incentives may aid in coronavirus vaccine distribution. But many employers are concerned about the liability they could create in offering such incentives, the letter said.
The signees asked EEOC to clarify how they might offer vaccination incentives without infringing upon the boundaries established by the Americans with Disabilities Act and other laws enforced by the agency. Specifically, the groups requested that the agency issue guidance that defines “what qualifies as a permissible incentive as broadly as possible.” An EEOC spokesperson said the agency appreciates “input from all stakeholders and will review the letter carefully.”
From the seeking public comment front —
- The National Committee for Quality Assurance is seeking “feedback on proposed new measures, changes to existing measures and proposed measures for retirement. Public comment is now open for HEDIS® Measurement Year 2022.” The public comment deadline is March 11, 2021.
- HHS’s Agency for Healthcare Research and Quality “encourage [interested parties] to review the draft report [titled “Strategies to Improve Patient Safety: Draft Report to Congress for Public Comment and Review by the National Academy of Medicine”] and send comments to PSQIA.RC@ahrq.hhs.gov no later than Feb. 16. We’ll review feedback in developing a final report for Congress later this year.” That’s not much time as the notice was posted today.