Weekend Update / Monday Roundup

The Senate will and the House of Representatives will be engaged only in Committee business this coming week.
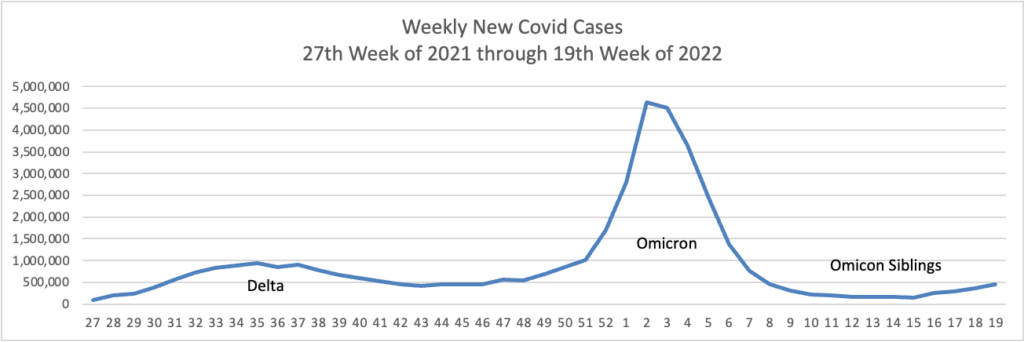
From the Omnicron and siblings front —
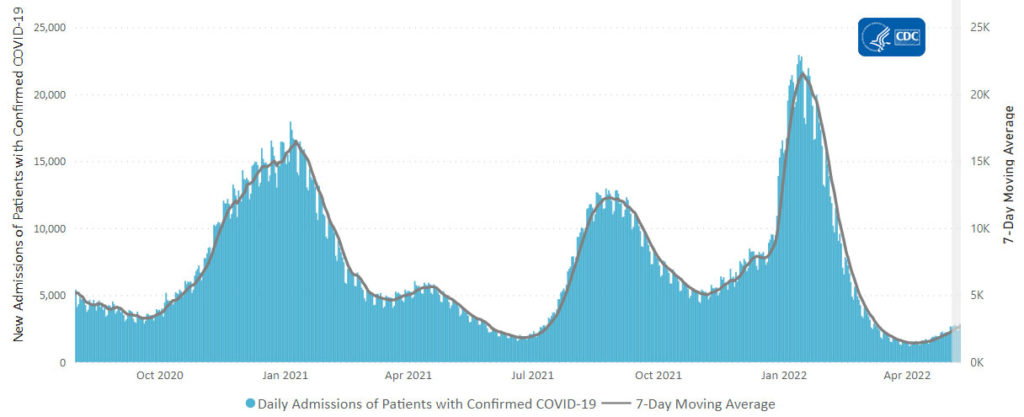
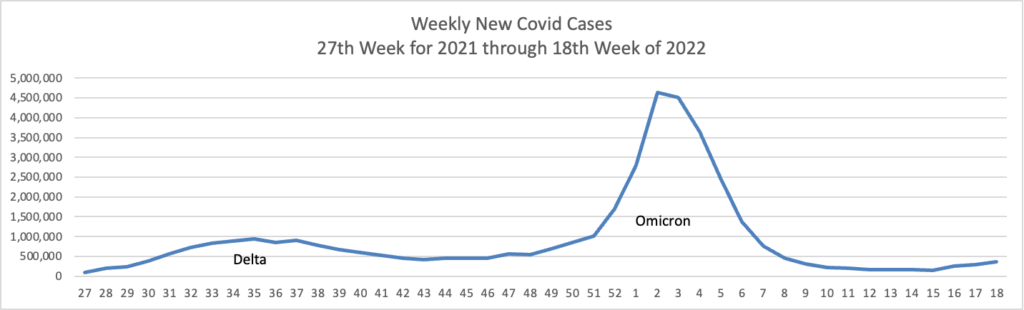
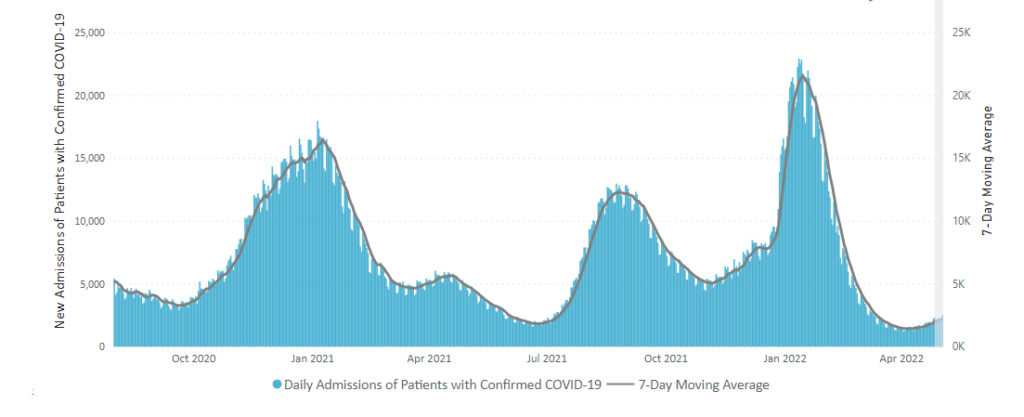
- Fortune reports “The U.S. is experiencing a sixth wave of COVID, with over 90,000 confirmed new cases a day and a 20% increase in hospitalizations over the past two weeks. The actual number of new cases per day likely sits at a half-million or more, “far greater than any of the U.S. prior waves, except Omicron,” writes Dr. Eric Topol, the executive vice president of Scripps Research and a professor of molecular medicine, in a recent blog post on the maps.” It’s hard to argue against this point.
- Bloomberg Prognosis offers a useful Q&A on when you can back to life after a case of Omicron. Here is a link to the CDC’s guidelines on isolation and quarantine due to Omicron.
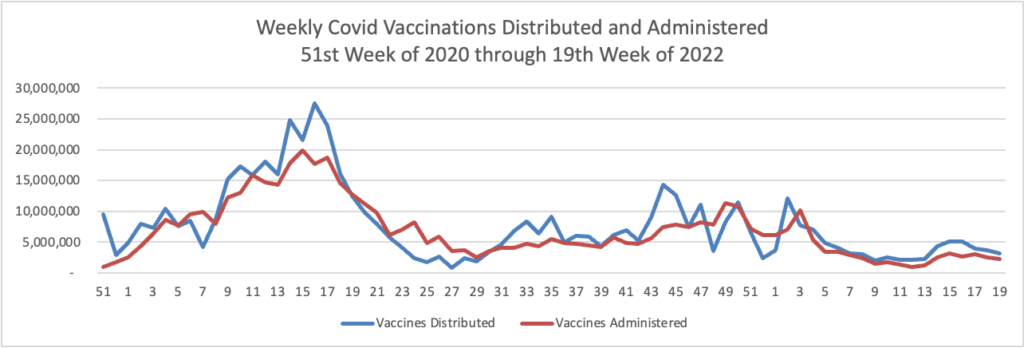
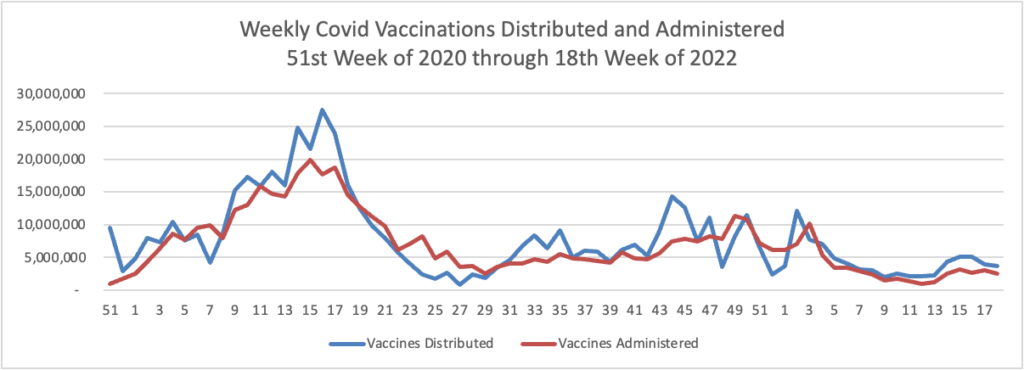
- The FEHBlog noticed that 75% of the American population age 12 and older is fully vaccinated against Covid.
- The American Medical Association discusses how Covid telemonitoring sets the model for other acute conditions.
From the Aduhelm front, the Wall Street Journal reports
The commercial failure of Biogen Inc.’s drug Aduhelm is putting new focus on the state of research into the causes of Alzheimer’s disease.
More than six million people in the U.S. are living with the progressive type of dementia, according to the Alzheimer’s Association, an advocacy group.
Aduhelm was hailed as a potential blockbuster that targeted a root cause of the disease by clearing a sticky protein known as amyloid from the brain. Abnormal accumulations of amyloid called plaque and tangles of another protein known as tau are characteristic features of the brains of people with Alzheimer’s.
“If you cut the brain open and amyloid plaque is absent, Alzheimer’s was not the cause of disease,” said Jeffrey Cummings, director of the Chambers-Grundy Center for Transformative Neuroscience at the University of Nevada, Las Vegas.
But research into the benefits of targeting amyloid in Alzheimer’s patients has been mixed. There are more questions than answers about the role amyloid plays in the development of the disease, neurologists say.
“Alzheimer’s is a complex disease. It’s unlikely that a single mechanism is contributing to it,” said Maria Carillo, the Alzheimer’s Association’s chief science officer. * * *
More than 140 drugs are in the pipeline as potential Alzheimer’s treatments, including drugs that target tau and microglia function, according to a survey of registered clinical trials in the U.S. Three other amyloid-targeting monoclonal antibodies, which are in the same class as Aduhelm, are in development. One, called lecanemab, was submitted this month by co-developers Biogen and Japan-based Eisai Co. to the Food and Drug Administration for potential approval.
Time will tell.
From the preventive care wellness front —
- Medscape reports an “alarming increase in esophageal cancers in middle-aged adults. The study’s author, Bashar Qumseya, MD, MPH, recommends that people with multiple risk factors for these cancers, i.e., obesity, diet, and gastroesophageal reflux disease, should undergo an endoscopy at the time of their first colonoscopy at age 45.
- The American Medical Association identifies steps that patients can follow to reverse pre-diabetes.
- Fortune Well offers helpful articles on how to unwind without alcohol and how companies can normalize menopause at work.
The FEHBlog just discovered that the Weekend Update did not go out on Monday morning. So here are Monday’s items that normally would have been posted in the Monday Roundup —
More from the Omicron and siblings front —
BioPharma Dive reports
Three doses of Pfizer and BioNTech’s COVID-19 vaccine met the Food and Drug Administration’s bar for success in a trial studying the shot in children younger than 5 years old, the companies said Monday. The FDA has tentatively scheduled a meeting of outside advisers to review the data in three weeks.
The agency delayed review of the vaccine in the youngest children earlier this year after a December review of data indicated a two-shot series didn’t spur an immune response that was likely to protect against disease. When Pfizer and BioNTech disclosed that data, they announced plans to test immune response and efficacy after three shots.
The announcement comes days after U.S. officials warned of a new surge of COVID-19 cases as mask mandates have been lifted and while immunity from vaccination and previous infections wanes. The FDA has granted emergency use authorization for as many as four shots of Pfizer and BioNTech’s vaccine — an initial two-dose series followed by two periodic boosters — for adults at least 50 years old.
Reuters adds U.S. “Health officials are considering extending the eligibility for a second COVID-19 vaccine booster dose to people under 50 amid a steady rise in cases, with the United States seeing a threefold increase over the past month.”
Bloomberg Prognosis recommends carrying around a portable carbon dioxide monitor to help prevent Covid or at least remind you to mask up and / or move along:
Carbon-dioxide monitors can assess how Covid-risky a space is because they help tell you whether you’re breathing in clean air. They measure the concentration of carbon dioxide, which people exhale when they breathe, along with other things like, potentially, virus particles. The more well-ventilated a space, the lower the reading on my monitor’s screen — meaning not only less carbon dioxide but also less of the stuff like Covid that might make people sick.
One place I didn’t expect this to be an issue was airplanes, because you hear so much about their top-of-the-line air quality systems. But in fact, some of the highest carbon dioxide readings on my travels were taken on flights, specifically during the boarding process.
It turns out that during boarding and deplaning, air systems aren’t typically running. Those periods are risky because people are mingling more than they do during a flight, says Joe Allen, an associate professor at the Harvard T.H. Chan School of Public Health who carries around his own CO2 monitor.
“We’ve been warning about this,” Allen says.
Fresh air is important for our health in ways that go well beyond Covid, but it’s also largely invisible. Carbon-dioxide monitors can change that.
What will they think of next?
The FEHBlog confesses that he took his eye off the flu virus this year. Beckers Hospital Review informs us “The CDC estimates there have been at least 6.7 million flu illnesses, 69,000 hospitalizations and 4,200 flu-related deaths so far this season.”
In other virus news, Reuters reports “Infection with adenovirus, a common childhood virus, is the leading hypothesis for recent cases of severe hepatitis of unknown origin in children that have led to at least six deaths, U.S. health officials said on Friday [May 20]. Furthermore,
The Centers for Disease Control and Prevention (CDC) said it is continuing to investigate whether 180 cases identified in 36 states and territories since last October represent an increase in the rate of pediatric hepatitis or whether an existing pattern has been revealed though improved detection.
From the mental healthcare front, Fierce Healthcare tells us
Mental health concerns are on the rise among teens, and the impact on parents and families is an unmet need employers could address, new data from Cigna’s Evernorth show.
The pandemic has significantly worsened mental health among teens and young adults, with 25% experiencing depressive symptoms and 20% experiencing anxiety symptoms, a JAMA study shows. About 80% of the 1,000 parents included in Cigna’s survey said their children are struggling with their mental health.
Nearly one-fifth (18%) of parents say their child’s needs are negatively impacting their job performance and productivity, according to the survey. In addition, 55% said they do not have enough support from their employer, and 1 in 7 said they were forced to leave or stay out of the workforce to manage their teenager’s needs.
“I think there’s going to be a long tail for these kids and also their family members,” Stuart Lustig, M.D., national medical executive for behavioral health at Evernorth, told Fierce Healthcare. “I think we’re in this for the long haul.”