Friday Stats and More
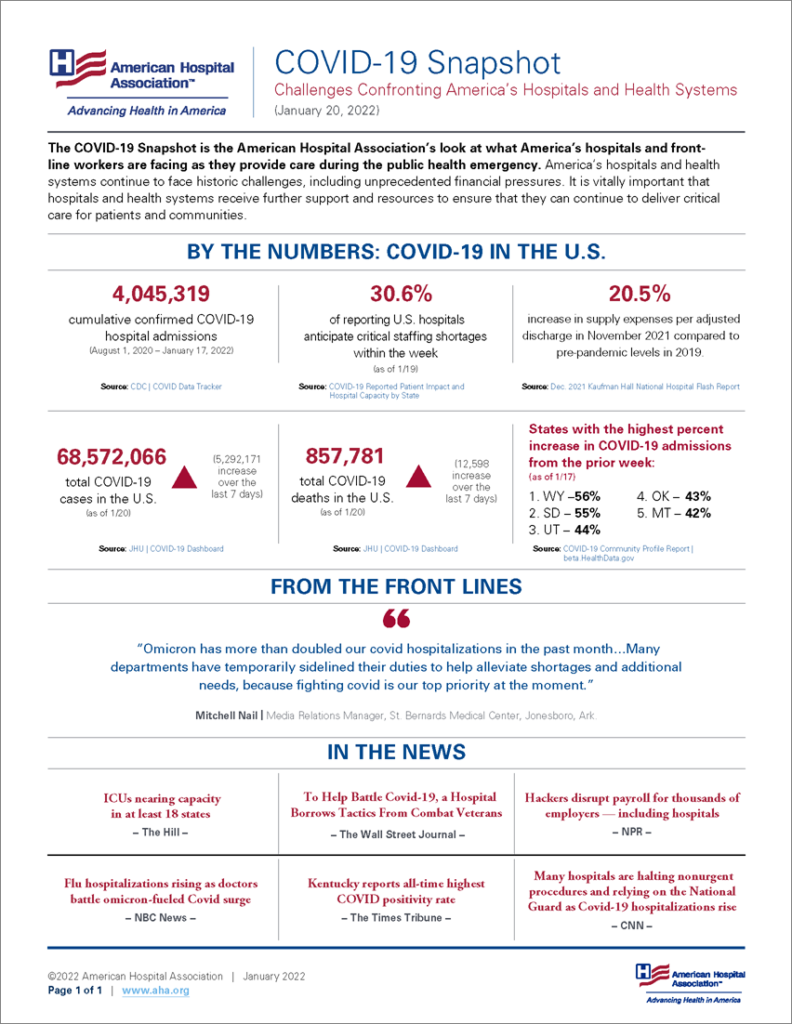
Based on the CDC’s Covid Data Tracker and using Thursday as the first day of the week, here is the FEHBlog’s weekly chart of new Covid cases from the 27th week of 2021 through the third week of 2022:

My word, could that be a cresting of the Omicron surge as discussed in this week’s posts?
The FEHBlog’s weekly chart of new Covid deaths has bounced up and down after climbing to just over 10,000 weekly deaths during the Delta surge. .

Last but not least here is the FEHBlog’s weekly chart of new Covid vaccinations distributed and administered from the 51st week of 2020 through the third week of 2022.

Here are links to the CDC’s Covid data tracker weekly review and its weekly Fluview.
In other COVID vaccination news —
- The Wall Street Journal reports that
Vaccines and booster shots offer superior protection from the Delta and Omicron variants, according to three new studies released by the Centers for Disease Control and Prevention.
The data back up earlier findings supporting booster shots and offer the first comprehensive insight into how vaccines fare against the Omicron variant. In one of the studies published Friday, a CDC analysis found that a third dose of either the vaccine from Pfizer Inc.and BioNTech SE or Moderna Inc. was at least 90% effective against preventing hospitalization from Covid-19 during both the Delta and Omicron periods.
The American Hospital Association adds
According to data from 25 state and local health departments, adults who were unvaccinated against COVID-19 as the omicron variant emerged in December had nearly three times higher risk of infection than adults fully vaccinated against COVID-19 and five times higher risk than adults who had received a booster, the Centers for Disease Control and Prevention reported today. The highest impact of COVID-19 booster doses compared with full vaccination was recorded among persons aged 50 and older. Because of reporting lags, the influence of the omicron variant on COVID-19-associated deaths could not be evaluated by vaccination status in December, the authors note.
- Medscape informs us that
The FDA could authorize Pfizer’s COVID-19 vaccine for children under age 5 in the next month, Anthony Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, said Wednesday.
“My hope is that it’s going to be within the next month or so and not much later than that, but I can’t guarantee that because I can’t out-guess the FDA,” he said during an interview with Blue Star Families, a nonprofit group that supports military families.
The younger age group will likely need three vaccine doses, he said, since two shots didn’t provide enough of an immune response during Pfizer’s clinical trials for kids ages 2-4.
In Covid vaccine mandate news, Govexec tells us
A federal court in Texas has issued an injunction against President Biden’s COVID-19 vaccine mandate for the federal workforce, pausing implementation of a requirement for more than 2 million civilian servants.
The Biden administration has already had sweeping success with the mandate, as most agencies have seen virtually their entire workforces come into compliance. Still, federal offices across the country were just beginning to move forward with suspensions—which could eventually result in firings—for those who did not meet the requirements. Biden issued the mandate by executive order in September.
Judge Jeffrey Brown, appointed by President Trump to the U.S. Court for the Southern District of Texas, said the case was not about whether individuals should be vaccinated or even about federal power generally.
“It is instead about whether the president can, with the stroke of a pen and without the input of Congress, require millions of federal employees to undergo a medical procedure as a condition of their employment,” Brown wrote. “That, under the current state of the law as just recently expressed by the Supreme Court, is a bridge too far.”
The Justice Department has appealed the decision to the U.S. Court of Appeals for the Fifth Circuit. The FEHBlog expects that the Fifth Circuit will lift the stay as soon as this weekend. The Society for Human Resource Management offers a helpful article for employers trying to keep track of the vaccine mandate decisions from the courts.
In other COVID vaccine mandate news, the Labor Department’s Wage and Hour Division announced today that
Employees [who are not exempt from the Fair Labor Standards Act] must be paid for time spent going to, waiting for, and receiving medical attention required by the employer or on the employer’s premises during normal working hours. Therefore, if an employer requires an employee to obtain a COVID-19 vaccine dose, undergo a COVID-19 test, or engage in a COVID-19 related health screening or temperature check during the employee’s normal working hours, the time that the employee spends engaged in the activity is compensable. Employees must be paid for such time during normal working hours, regardless of where the activity occurs. This is true regardless of whether the employer is subject to the OSHA Vaccination and Testing ETS.
In Covid treatment news, the Food and Drug Administration announced today that the agency “took two actions to expand the use of the antiviral drug Veklury (remdesivir) to certain non-hospitalized adults and pediatric patients for the treatment of mild-to-moderate COVID-19 disease. This provides another treatment option to reduce the risk of hospitalization in high-risk patients. Previously, the use of Veklury was limited to patients requiring hospitalization.”
From the Covid OTC testing coverage mandate department, the Kaiser Family Foundation has surveyed the coverage approaches of 13 large health insurers. Don’t blame the insurers on this one because health insurers don’t typically cover OTC products and the government only allow four days to implement the mandate.
From the and more department
- In telehealth news, mHealth Intelligence tells us that
Telehealth utilization peaked in the first half of 2020 and decreased as the year came to a close, with providers predicting that virtual care use would continue to decline in upcoming years, according to the 2021 Medical Group Telehealth Survey.
AMGA Consulting conducted the survey and gathered responses from 56 medical groups representing more than 38,000 healthcare providers.
The majority of the participants (86 percent) were part of multispecialty groups with primary care, while the remaining were either multispecialty without primary care, primary care, or single-specialty groups. * * *
The survey results suggest that although telehealth use skyrocketed during the COVID-19 pandemic, virtual care may see the most success with patients who prefer the modality over in-person care or whose health concerns can be easily addressed virtually.
The FEHBlog remains a strong proponent of hub and spoke telehealth for mental health care because every televisit is in network.
- The American Hospital Association informs us that “The Department of Health and Human Services’ Office of the National Coordinator for Health Information Technology seeks comments through March 25 to inform potential future rulemaking on how the ONC Health IT Certification Program could incorporate standards, implementation specifications and certification criteria to reduce the burden of prior authorization.”
- The Congressional Budget Office released a report titled “The Prices That Commercial Health Insurers and Medicare Pay for Hospitals’ and Physicians’ Services.”
CBO examined potential explanations for why the prices paid by commercial insurers are higher and more variable than those paid by Medicare FFS. CBO’s analysis and literature review suggest the following conclusions:
— Greater market power among providers consistently leads to prices for commercial insurers that are higher than Medicare FFS’s prices and that vary more widely, both among and within areas. Hospitals and physicians’ groups may have market power because they have a dominant share of the market in an area or because an insurer sees them as essential to its network of providers.
— Some of the variation in the prices that commercial insurers pay for hospitals’ and physicians’ services is explained by differences in the prices of inputs needed to deliver those services.
— Higher hospital quality is associated with higher prices paid by commercial insurers, although whether there is a causal link between quality and prices, and the direction of any such link, is not clear.
— The share of providers’ patients who are covered by Medicare and Medicaid is not related to higher prices paid by commercial insurers. That finding suggests that providers do not raise the prices they negotiate with commercial insurers to offset lower prices paid by government programs (a concept known as cost-shifting).
- Healthcare Dive informs us that
IBM is selling the data and analytics assets of its Watson Health business to a private equity firm as it looks to refocus on its core cloud business.
The sale, which is expected to close in the second quarter this year has been anticipated for quite some time, and comes following the limited success of Watson Health, despite a spate of high-profile acquisitions of health information companies to bolster the enterprise.
Financial terms of the deal were not disclosed.
- OPM announced today that
[F]ederal civilian employees in the U.S. will now be paid at least $15 per hour.
OPM issued a memorandum for heads of Executive departments and agencies that provides implementing guidance for how agencies should adjust pay rates for General Schedule (GS) and Federal Wage System (FWS) employees stationed in the U.S., and how to use administrative authority for other pay systems to lift the pay of federal employees who currently make less than $15 per hour. In total, these changes will impact 67,000 out of 2.2 million federal employees. The largest share of these workers, over 56,000 of them, currently work at the Department of Defense. OPM’s guidance directs agencies to implement these changes by January 30, 2022
- To tide you over the weekend, here is a link to Healthcare Dive’s Deep Dive on four 2022 key trends for providers and payers.