Weekend Update

The House of Representatives and the Senate will be engaged in Committee business and floor voting this coming week.
From the Omicron and siblings front —
Bloomberg Prognosis offers an interesting observation from Katrine Wallace, an epidemiologist at the University of Illinois at Chicago,
“For some viruses, where there is better mucosal immunity in the nose (via past infection or vaccines), people can fight off pathogens and develop an immune response without ever feeling ‘sick.’” In other words, for certain infections, your immune system might get revved up by recognizing a virus, and then swiftly fight it off.
“However, Covid-19 is not a virus that we have developed lasting mucosal immunity for, either through vaccines or via previous infections,” says Wallace.This is the whole rationale for the development of the new Covid shots that are inhaled instead of injected, she says. The nose and mouth are where Covid first enters the body, so the vaccine antibodies elicited by those types of vaccines give people a more immediate line of defense.
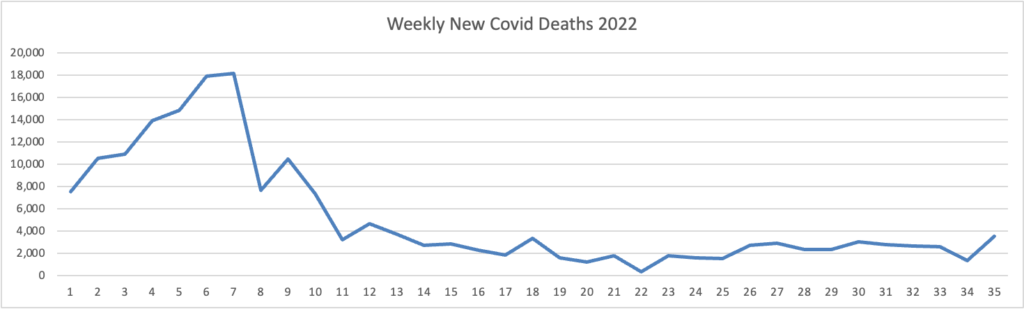
The Wall Street Journal provides details on nagging Covid death levels:
Roughly 85% of people who died from Covid-19 through mid-August this summer were 65 or older, a Wall Street Journal analysis of death-certificate data show. The rate is similar to 2020 peaks, before vaccines were available. Deaths trended younger for much of last year.
Covid-19 is on pace to be the third-leading cause of death for the third straight year, said Dr. Robert Anderson, chief of the mortality statistics branch at the CDC’s National Center for Health Statistics. Since 2020, it has trailed only heart disease and cancer, significantly reducing life expectancy. * * *
The health system AdventHealth counted 24 deaths related to Covid-19 at its Orlando, Fla.-area hospitals in August. Age was the biggest factor, although younger patients with compromised immune systems were also at risk, doctors with the health system said. All but one Covid-19 patient who died had serious health problems such as diabetes, chronic obstructive pulmonary disease, heart failure and obesity.
Unfortunately, the Journal’s article discusses vaccination status but does not factor in the Paxlovid pill or other available treatments, which should be a game changer for older folks with Covid.
From the mental healthcare front — ‘
Yesterday, September 10, was World Suicide Awareness Day. McKinsey and Company reported,
The suicide rate in the United States has risen over the past 20 years to become the second-leading cause of death for people between the ages of ten and 34, write partner Erica Hutchins Coe, senior partner Martin Dewhurst, senior partner Tom Latkovic, and co-authors in a recent report from the McKinsey Health Institute (MHI). And by winter of 2021, the weekly rate of ER visits by adolescents who attempted suicide was 39 percent higher than pre-pandemic levels. By taking action to address this urgent public health issue, organizations, educators, healthcare professionals, governments, and society at large could help millions in crisis. This #WorldSuicidePreventionDay, learn about ongoing efforts by MHI and its collaborators to improve crisis care in the United States * * * .
The article provides links to relevant McKinsey publications on this important topic.
The American Medical Association’s “What Doctors Wish Their Patients Knew” column delves into loneliness and health.
From the social determinants of health front, Fierce Healthcare looks into CVS’s Healths efforts to improve health equity.
When the CVS Caremark team geared up to take on health disparities, it quickly realized that any initiative would require a significant basis in data to succeed.
That entailed both gathering more data and building the tools necessary to track and analyze them. For example, Joel Helle, vice president of physician services at CVS Specialty, told Fierce Healthcare that Caremark has not historically gathered race and ethnicity data, but now asks payers and plans sponsors for that information to more accurately target where disparities are occurring.
“It’s real race and ethnicity data, and we know who those patients are,” he said. “That’s the future, in my mind, of what everybody needs to do.”
In addition, the company built a proprietary tool that combs data from 17 different indexes to identify where disparities exist, he said. That tool, he said, puts “red dots” on the map to highlight risks, and the Caremark team can then use its internal data to further drill down to challenges in specific communities.